

Background
Endocrine paraneoplastic syndromes occur when tumors acquire the ability to produce bioactive substances unrelated to their tissue of origin. Common paraneoplastic syndromes involve the secretion of parathyroid hormone-related peptide (PTHrP) causing hypercalcemia, antidiuretic hormone (ADH) causing hyponatremia, and adrenocorticotrophic hormone (ACTH) causing Cushing’s syndrome (CS). These endocrine paraneoplastic syndromes often occur in highly malignant tumors and are most commonly associated with lung cancer.1 Here, we discuss the case of a patient who presented with ectopic Cushing’s syndrome as the first manifestation of metastatic small cell lung carcinoma (SCLC).
Case Presentation
A 67-year-old man with a history of hypertension, hyperlipidemia, and coronary artery disease presented to the emergency department with several days of fatigue and generalized weakness. He had a remote 5 pack-year smoking history. He denied any fever, chills, night sweats, changes in weight, cough, or shortness of breath. He had no prior history of diabetes or hypertension. He had seen his primary care physician about two weeks prior to admission because his wife had noticed a new tremor, difficulty with word finding, and new lower extremity edema. At that time, he was also noted to have mildly elevated fasting glucose. He was started on furosemide for the management of lower extremity edema.
On presentation to the hospital, his temperature was 97.1°F, heart rate 100 bpm, blood pressure 144/81 mmHg, respiratory rate 18, and oxygen saturation 96% on room air. He was well-appearing and in no acute distress. The physical exam was remarkable for jaundice, scattered ecchymoses, and a mild tremor. He had no evidence of facial plethora, striae, truncal obesity, or muscle wasting.
Labs were notable for potassium 1.9 mEq/L (3.6-5.1mEq/L), VBG pH 7.65 / pCO2 48 mm Hg, bicarbonate 45 mEq/L (22-32 mEq/L), creatinine 1.30 mg/dL (from baseline 1 mg/dL), glucose 231 mg/dL (67-99 mg/dl), AST 58 IU/L (10-42 IU/L), ALT 77 IU/L (6-45 IU/L), ALP 141 IU/L (34-104 IU/L), total bilirubin 6.4 mg/dL (0.2-1.3 mg/dl), WBC 17.4 x109/L (3.5-11 x 109/L), hemoglobin 15.9 g/dL (13.5-16 g/dl), and platelets 104 x109/L (150-400 x 109/L). Chest X-ray revealed right hilar enlargement. A chest, abdominal, and pelvic computerized tomography (CT) scan demonstrated a 6.9 cm right mediastinal mass compressing the mainstem bronchus, mediastinal lymphadenopathy, innumerable hepatic metastases, and an enlarged 5.3 cm heterogeneous appearing left adrenal gland concerning for metastatic disease (Figures 1 & 2).
_lung_window_and_b)_mediastinal_window_of_ct_chest_showing_a_new_6.9_cm_mediastinal_mass.png)

Given his hypokalemia, metabolic alkalosis, and imaging findings concerning for malignancy, a midnight serum cortisol was checked; this was >75 mcg/dL, the upper limit of reporting for our laboratory. Adrenocorticotropic hormone was elevated at 380 pg/mL, and aldosterone was low-normal at 8.5 ng/dL. Cortisol levels remained unsuppressed by both low- and high-dose dexamethasone suppression tests (DST). MRI brain was negative for pituitary mass. A liver biopsy was obtained, confirming metastatic small-cell lung carcinoma. Spironolactone and ketoconazole were initiated. The patient’s cortisol levels began to downtrend, and his metabolic abnormalities normalized. He was transferred to the oncology floor for inpatient initiation of palliative carboplatin. Unfortunately, the patient developed aspiration pneumonia complicated by hypoxic respiratory failure and passed away a few days after the initiation of chemotherapy.
Discussion
In ectopic ACTH syndrome, a non-pituitary tumor secretes high levels of ACTH, leading to an endogenous state of hypercortisolism. About 5-10% of CS cases are caused by ectopic ACTH production.2 SCLC is most commonly implicated, accounting for up to three-fourths of all cases. It is followed by neuroendocrine tumors, pheochromocytomas, and medullary thyroid carcinomas.3,4 Up to 20% of ACTH-secreting tumors remain unidentified despite repeated imaging.2 Some studies also suggest that SCLC patients with adrenal metastases, such as our patient, may have a greater propensity to develop hypercortisolism, as there is increased cortisol production in areas adjacent to the ACTH-producing adrenal tumor.5
Aggressive cancers like SCLC produce ACTH at much higher rates than pituitary adenomas.2 Many patients will not have had time to develop the exam findings of chronic Cushing’s, such as truncal obesity, buffalo hump, moon facies, and proximal muscle wasting.6 Instead, as seen in our case, they may present acutely with features of severe hypercortisolism, including muscle weakness, hyperglycemia, hypertension, hypokalemia, and metabolic alkalosis. The last three are driven by activation of the mineralocorticoid receptor by excess cortisol, leading to pseudohyperaldosteronism.
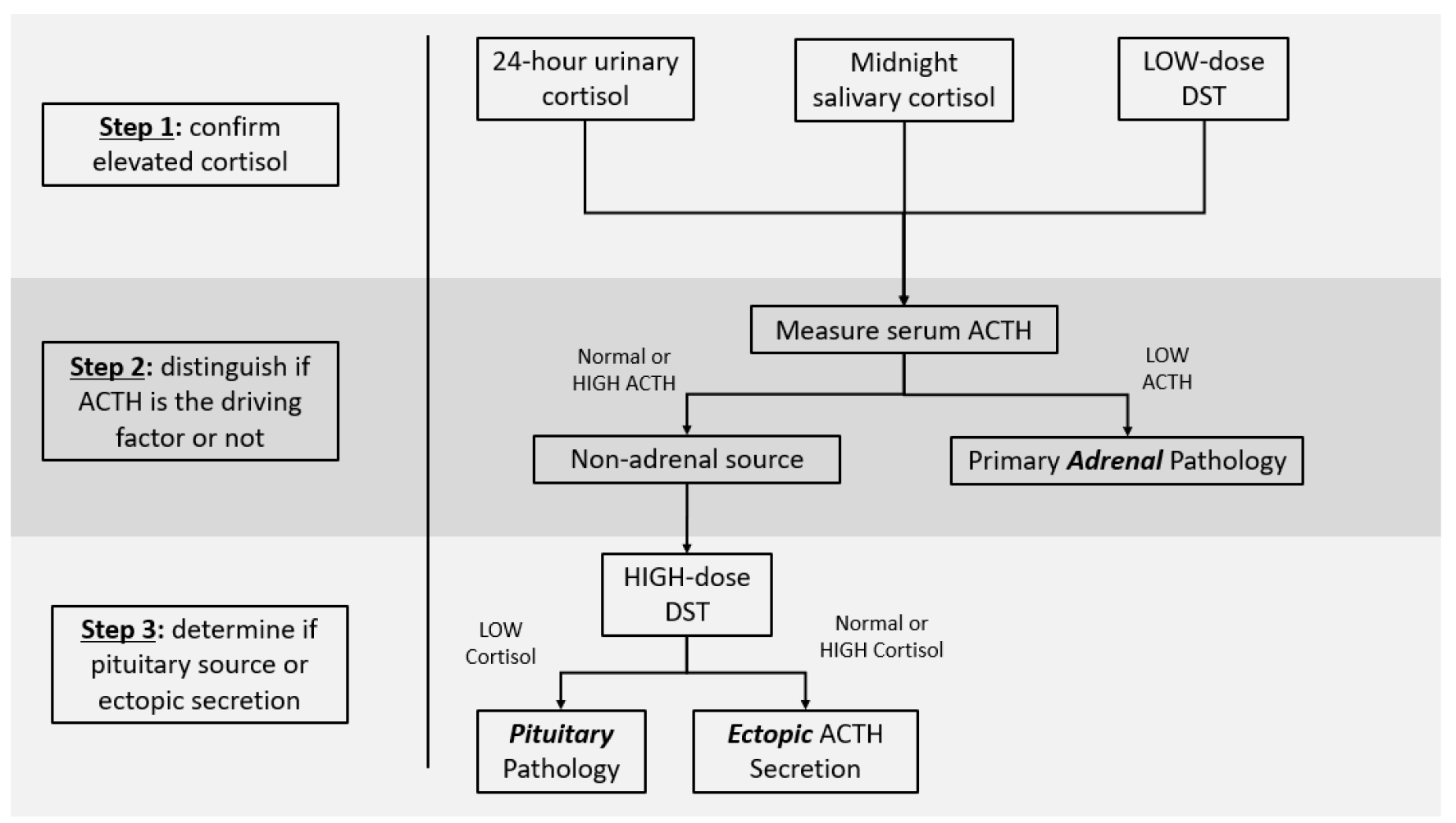
The first step in diagnosis is confirming endogenous cortisol overproduction with 24-hour urinary cortisol, midnight salivary cortisol, or low-dose dexamethasone suppression testing. Next, ACTH is measured; elevated or inappropriately normal levels rule out primary adrenal disease. Finally, the high-dose dexamethasone suppression test is used to distinguish pituitary adenomas – which often retain some responsiveness to negative feedback mechanisms – from an ectopic source (Figure 3).2

ACTH production is a poor prognostic sign in SCLC, associated with more extensive disease and decreased response to first-line treatment.2 Estimated survival ranges from 3-6 months. Prompt diagnosis and treatment are essential to improve outcomes. Hypercortisolism can independently lead to increased mortality from cardiovascular and infectious complications. Treating the effects of hypercortisolism prior to initiating chemotherapy may contribute to an increase in survival time.7 Therefore, in addition to tumor-targeted therapy, treatment should include steroidogenesis inhibitors such as ketoconazole and metyrapone to suppress cortisol to normal levels rapidly.2,8
Author Contribution
All Authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures
The authors have no conflicts of interest to disclose.