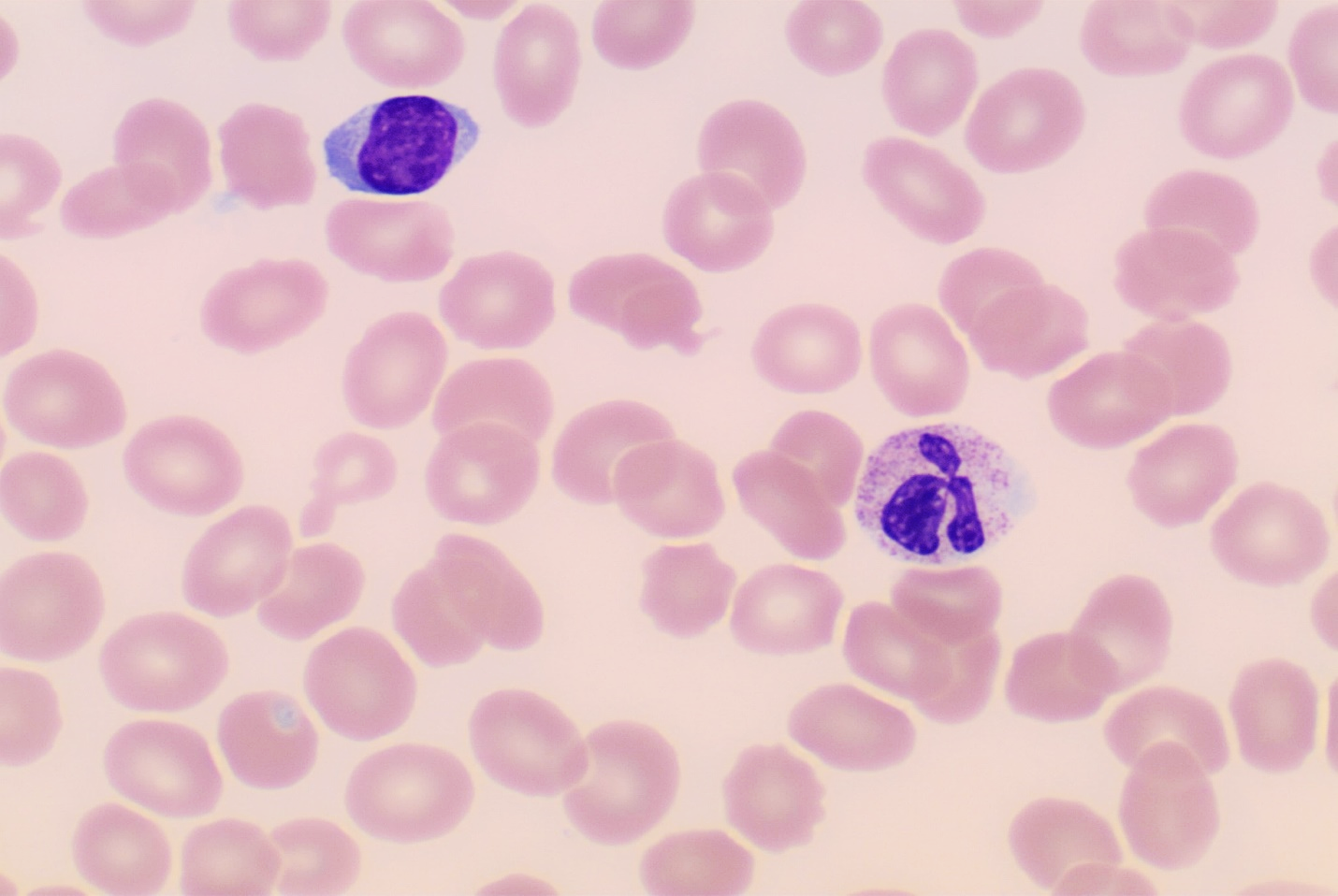
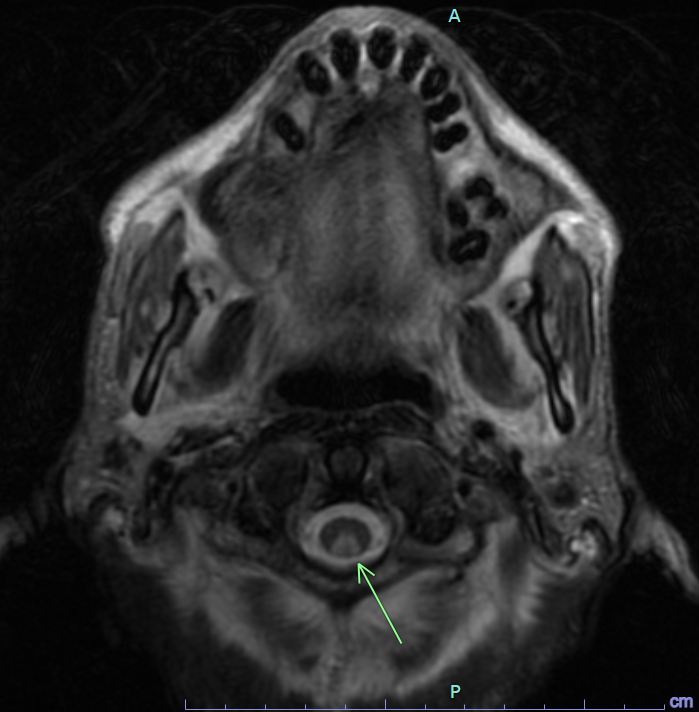
A 60-year-old patient presented with severe malnutrition and failure to thrive along with bilateral lower extremity weakness, cognitive dysfunction, and absent ankle reflexes on examination. He had macrocytic anemia with a mean corpuscular volume (MCV) of 117 fL . Vitamin B12 level was found to be less than 150 pg/mL (normal: 232-1245 pg/mL) with normal folate levels of 7.3 ng/mL (normal >4 ng/mL). Peripheral blood smear showed macrocytic normochromic red blood cells with mild anisopoikilocytosis and neutrophils with normal morphology (Figure 1). Magnetic Resonance Imaging (MRI) of the cervical spine with and without contrast showed a long segment mildly expansile cervical cord T2 signal hyperintensity predominantly involving the dorsal columns extending from the cervicomedullary junction to the C6 level measuring approximately 0.7 x 0.5 x 8.7 cm and associated diffusion restriction without enhancement (Figure 2). He was diagnosed with subacute combined degeneration of the cord due to Vitamin B12 deficiency, and was started on intravenous Vitamin B12 therapy. Further workup revealed a positive intrinsic factor blocking antibody suggesting pernicious anemia as the etiology.

_of_the_cervical_spine_showing_cervical_cord_t2_signal_hyp.png)
Subacute combined degeneration of the cord is characterized by degeneration of the dorsal columns and the lateral columns of the spinal cord due to demyelination.1 It is most commonly caused by a deficiency in vitamin B12.2 Other causes include gastric abnormalities (gastric surgery/autoimmune gastritis/pernicious anemia), small bowel abnormalities, pancreatic disease, drug-induced, and genetic abnormalities. Vitamin B12 is necessary for maintaining neuronal myelin integrity. It acts as a cofactor for enzymes involved in converting homocysteine to methionine and methylmalonyl-CoA to succinyl-CoA which is necessary for myelin synthesis.1 It commonly presents with sensory deficits, paresthesia, weakness, ataxia, and gait disturbance, and in severe cases can lead to spasticity and paraplegia.3 MRI of the spine shows a very typical pattern with T2 hyperintense signal alterations usually confined to the posterior columns, which may involve the lateral columns and rarely the brainstem.4,5 Subacute combined degeneration of the cord is treated with parenteral cobalamin which is administered at a dose of 1000mcg once a week for one month, followed by 1000mcg once every month until clinical response is obtained.1
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Sambhawana Bhandari
Department of Medicine,
Danbury Hospital, Nuvance Health, CT
Email: bhandarisambhawana@gmail.com
ORCID: 0000-0001-6446-0362