A 33-year-old female patient with history of anxiety presented for an episode of palpitations, chest pain (6/10 intensity), with decreased strength in the right side of the body, lasting approximately 15 minutes, without any other associated neurological symptoms. She denied having orthopnea, paroxysmal nocturnal dyspnea, or leg swelling. She was prescribed aspirin 81mg daily, rosuvastatin 20mg daily, and referred to get an echocardiogram done for suspected transient ischemic cerebrovascular disease.
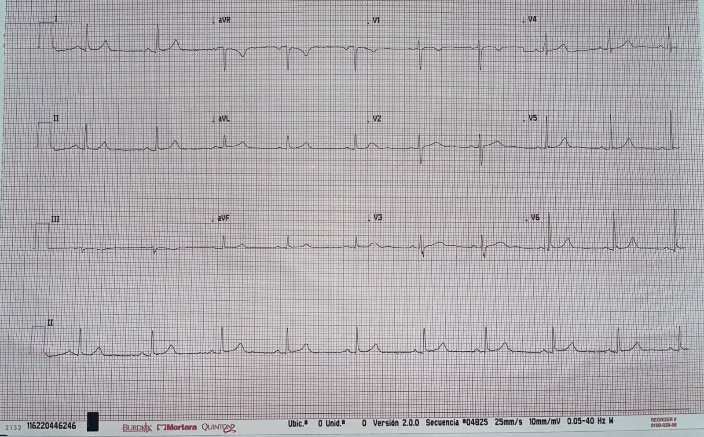
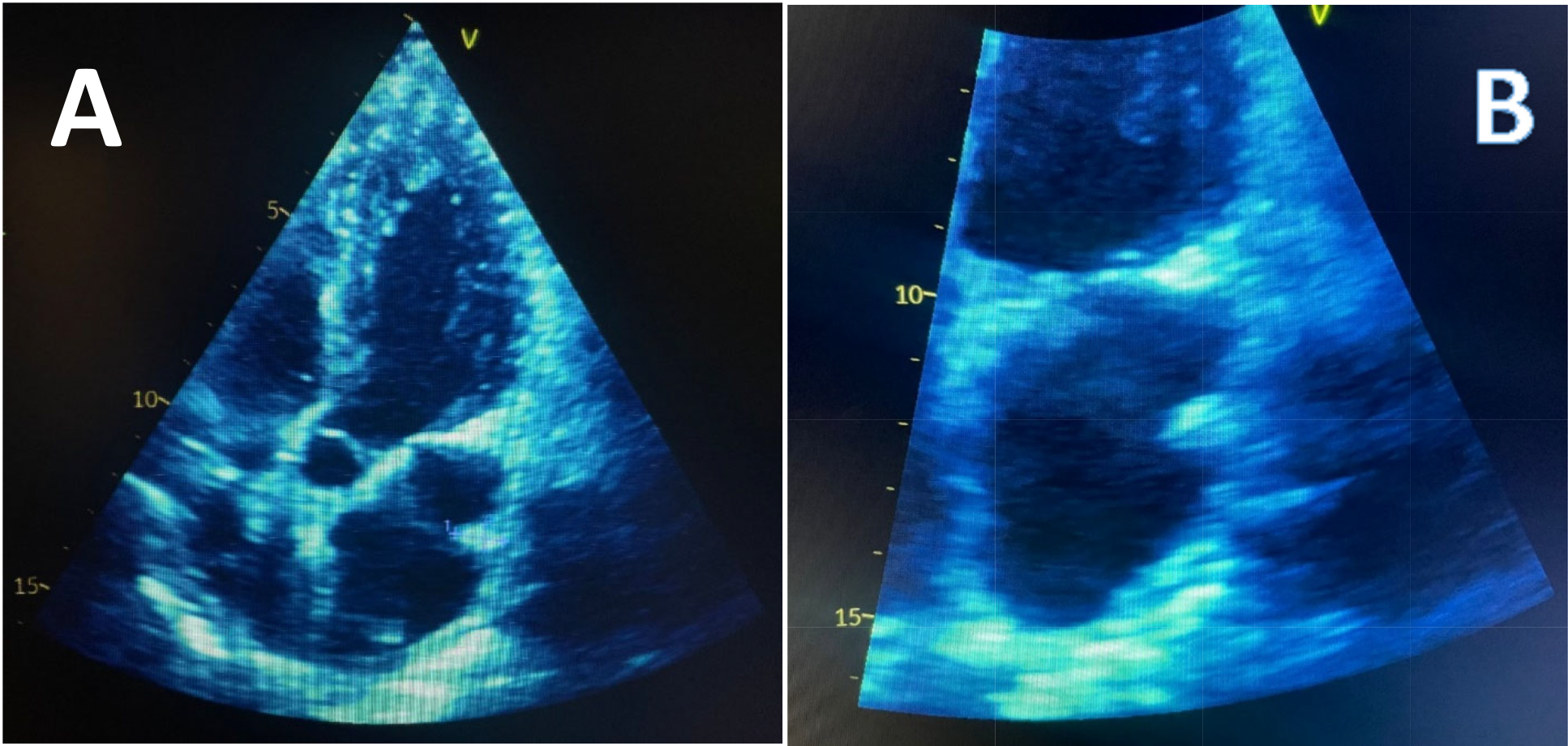
Physical examination showed blood pressure 110/60, pulse of 57bpm, and respiratory rate of 17 per minute. There was no jugular venous distention, well-ventilated lungs, normal cardiac sounds, no murmurs, and lower limbs without edema. The lipid profile was normal. An electrocardiogram was performed that showed sinus bradycardia with 57 bpm (Figure 1). Chest X-ray did not have any notable findings. A transthoracic echocardiography was performed. In the 4-chamber view, at the entrance of pulmonary veins, a pedicled hyperechoic image approximately 11x6mm projecting towards the lateral wall of the left atrium, corresponding to Coumadin ridge was identified (Figure 2). Her episode was ultimately attributed to anxiety, and her medications were discontinued. She was advised to start lifestyle changes and given a referral to psychiatry. CT Brain was not done since the patient did not present with any neurological signs at the time of physical examination and she only had transient right sided weakness lasting 15 minutes.

_4-chamber_projection_of_pedicled_hyperechoic_image_at_the_level_of_pulmonary_veins__pr.png)
Echocardiogram has drastically improved in terms of clarity and resolution and can now identify normal anatomical variants of the heart. The ridge may appear to be attached to the roof of the left atrial appendage with a rounded end extending towards the atrium, and often referred to as “Q-tip sign” on echocardiography.1 Due to its rounded edge, the coumadin ridge has often been falsely diagnosed as a thrombus, thereby, resulting in unnecessary anticoagulation with Coumadin (warfarin) and hence the name, “Coumadin ridge”.2 It is an embryological remnant similar to a band in the left atrium between the left upper pulmonary vein and the left atrial appendix, and is considered an anatomical variant, and if particularly prominent, it may be easily mistaken for a tumor such as an atrial myxoma or thrombus.3,4 The ridge contains the Marshall ligament, the autonomic nerve bundle and small artery of the atrial node, and noted to be more common in patients with atrial fibrillation.5,6 If coumadin ridge is seen on TTE and questions still remain about the diagnosis, a full-volume three-dimensional transthoracic echocardiography with color Doppler can provide additional clarity of the surrounding structures.7 Transesophageal echocardiography can also be performed, if necessary, as the Coumadin ridge is best seen using the midesophageal two-chamber view.7 In very difficult cases, a cardiac MRI can be done to provide clarity to the diagnosis. On both T1 and T2 weighted images, the Coumadin ridge should have the same signal strength as the adjacent cardiac tissue.3 In conclusion, coumadin ridge is a normal variant of the left atrium, and awareness of this diagnosis is essential to avoid putting patients through unnecessary interventions, both treatments and surgeries.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of interest
The authors declare that they have no conflict of interest.