BACKGROUND
Emphysematous cystitis is a rare and life-threatening entity that arising from complicated urinary tract infections seen primarily in patients with poorly controlled diabetes mellitus. It is characterized by intraluminal air in the bladder and bladder wall caused by fungal or bacterial fermentation of glucose in the urine. Certain common organisms associated with the disease include E. coli, K. pneumoniae, P. mirabilis, among others.1,2 Nonspecific signs and symptoms such as flank pain, vomiting, fever, dysuria, and urgency make diagnosing emphysematous cystitis a challenge, and delay in diagnosis and treatment can cause dissemination of the infection to the ureters and kidneys, increasing mortality.
CASE PRESENTATION
A 69-year-old male with a past medical history of benign prostatic hyperplasia and type II diabetes mellitus presented to the hospital for left-sided flank pain, gross hematuria, nausea, and vomiting that started one week prior. The patient has a history of tobacco use and recreational alcohol use. The patient had no recent procedures or instrumentation. The pain was intermittent, radiating to the left lower quadrant and pelvic area, and has worsened since the onset.
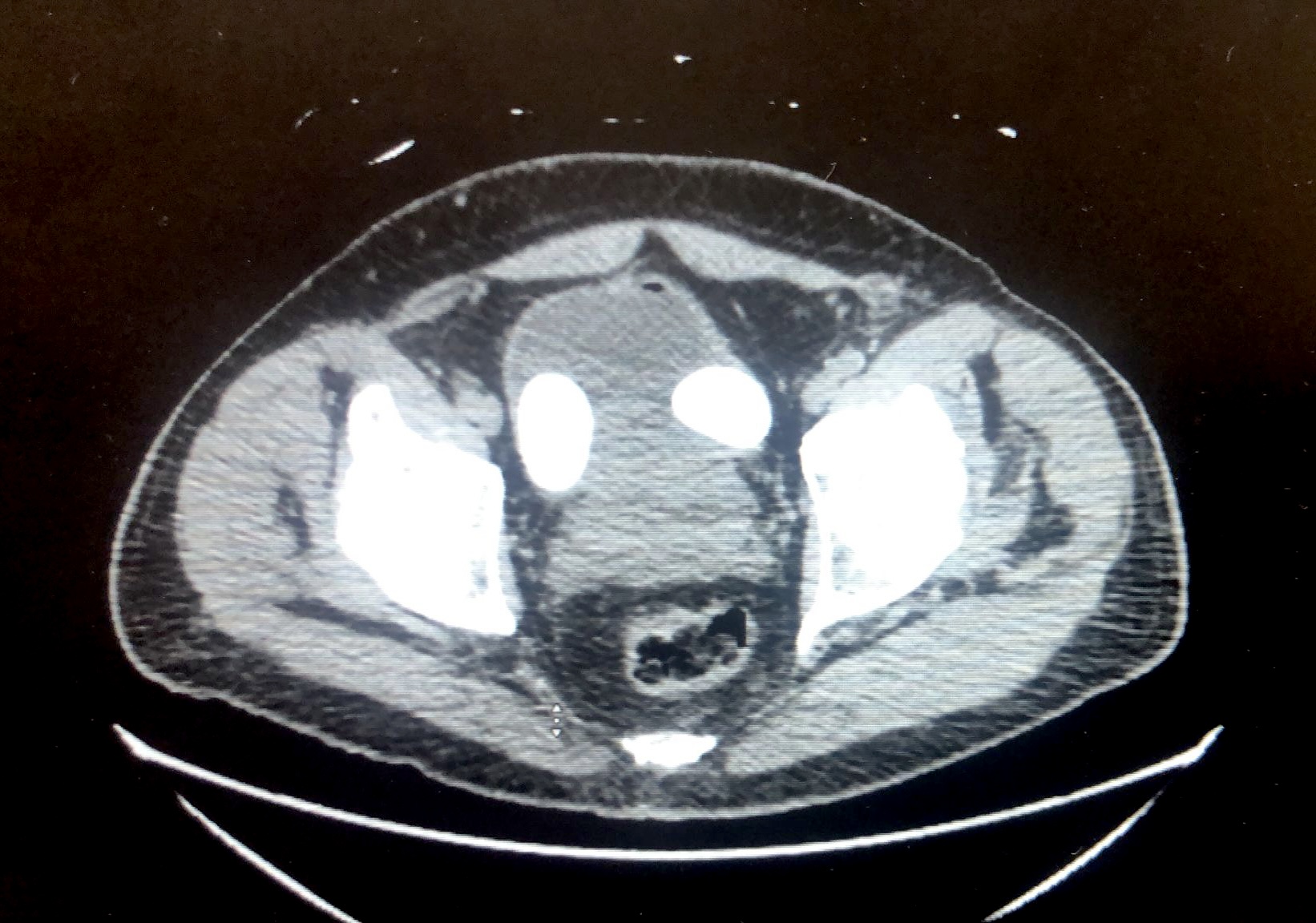
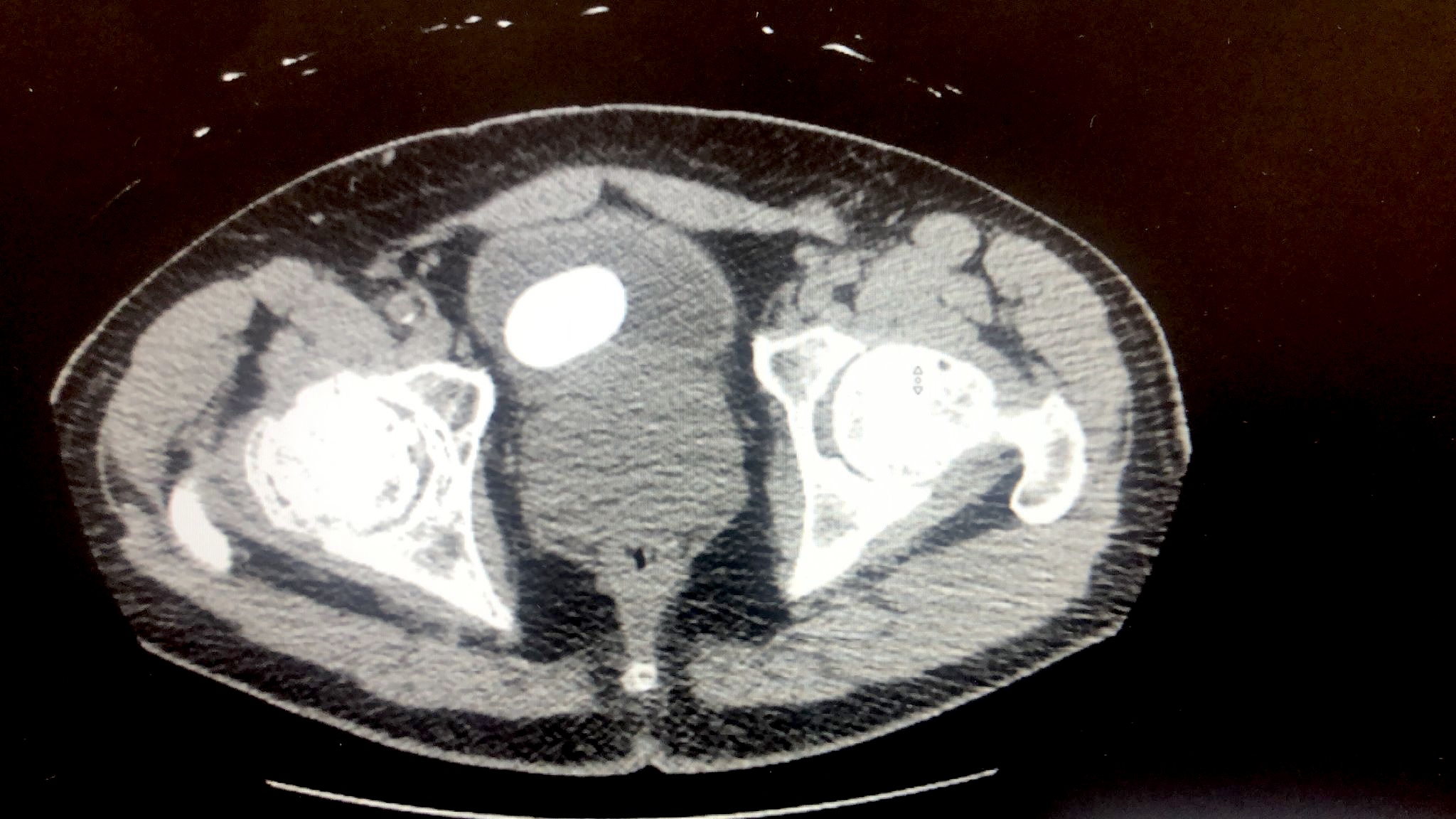
Upon arrival at the hospital, he was noted to be hypotensive, tachycardic, and febrile. Laboratory analysis showed leukocytosis, lactic acidosis, hyperglycemia of 204 mg/dL, and glycated hemoglobin of 8.2% (Table 1). Urine analysis was positive for bacteria, nitrates, leukocytes esterase, gross blood, and red blood cells with no casts. Computed tomography of the abdomen and pelvis without contrast revealed two large bladder stones measuring up to 4.5cm in diameter (Figure 1), trace intraluminal air in the bladder, and an enlarged prostate measuring 7.7 x 6.1 cm (Figure 2). Urine cultures grew Extended Spectrum Beta-Lactamase (ESBL) E. Coli, and the patient was started on Ertapenem. Moreover, strict glycemic control was prioritized in this patient, where his target glucose was to be maintained at less than 140mg/dl. The patient’s overall clinical status quickly improved after initiating antibiotic therapy and strict glucose control, and he was discharged with arrangements for outpatient bladder stone removal and a midline intravenous catheter to complete the antibiotic regimen.


DISCUSSION
Emphysematous cystitis is an uncommon and severe form of urinary tract infection characterized by the presence of gas within the bladder and its walls. The exact cause of emphysematous cystitis is not well understood. However, it is believed to result from the accumulation of gas produced by bacteria through the fermentation of sugar in the bladder’s submucosa and lumen. The most common organisms associated with emphysematous cystitis are E. coli and Klebsiella pneumoniae. Diabetes mellitus is a significant risk factor, with over 50% of patients having this condition.3 Toyota et al. found that diabetes was present in 66.7% of patients with emphysematous cystitis.4 Other risk factors include bladder outlet obstruction, -as the patient presented in this case- neurogenic bladder and being female. The severity of the disease varies, ranging from asymptomatic cases to life-threatening conditions such as septic shock. Pneumaturia, the passage of gas during urination, is a common symptom and should raise suspicion of emphysematous cystitis. Although, it can present asymptomatically or with classic Urinary Tract Infection symptoms.
Diagnosis is typically made through radiographic or computed tomographic imaging, which reveals the presence of gas within the bladder and its walls (CT preferred). It is essential to perform urine and blood cultures to guide appropriate antimicrobial therapy, as bacterial bloodstream infections are common. Procalcitonin, a biomarker for bacterial infection, can aid in assessing the severity of inflammation.3 Timely diagnosis is crucial for a favorable outcome, as a delay in treatment can contribute to the relatively high mortality rate of approximately 20% associated with this condition. If diagnosed on time, most cases of emphysematous cystitis can be treated and resolved with antibiotic treatment.
This case illustrates the importance of accurately diagnosing emphysematous cystitis, as it can become life-threatening if not adequately managed promptly. Often, this disease can be missed with primary imaging modalities such as X-rays and ultrasounds. The gold standard imaging study is Computed Tomography of the abdomen and pelvis with or without contrast. Immediate treatment with intravenous broad-spectrum antibiotics is needed to decrease the consequences of delayed diagnoses, such as bladder rupture and death.4 In addition, strict glucose control in these patients is crucial. It is imperative for physicians to recognize the detrimental effects of hyperglycemia and glucosuria that may impede the resolution of the disease.5 Hyperglycemia hinders the eradication of the infection, and extension into the ureters and kidneys can lead to significant complications such as emphysematous pyelonephritis, increasing mortality significantly. Therefore, it is vital to diagnose emphysematous cystitis and apply the proper management to improve patient outcomes substantially rapidly and appropriately.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Corresponding Author
Cinthia Reyes, M.D
Pontificia Universidad Católica Madre y Maestra School of Medicine
Autopista Duarte Km 1 1/2, Santiago De Los Caballeros 5100, Dominican Republic
Phone: +18294276761
Email: cinthiayamel@gmail.com