
Background
HACEK (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella) are gram negative organisms that are typically part of the oropharyngeal flora. Though not particularly pathogenic they can be a rare cause of endocarditis (approximately 1-3%) of cases. These organisms typically affect those with structural heart disease or prosthetic valves. Diagnosis is difficult as they have a subacute clinical course and was previously hard to culture due to their fastidious nature. In this case, we present an instance of multivalvular endocarditis caused by Aggregatibacter actinomycetemcomitans, which led to mechanical aortic valve dehiscence.
Case Presentation
A 36-year-old man with a history of congenital aortic valve stenosis, who had previously undergone two mechanical valve replacements, presented to the hospital with a two-week history of fever, chills, fatigue, generalized weakness, and malaise. The patient had his first aortic valve replacement at the age of 17 and a subsequent redo surgery at the age of 34 due to restenosis and severe regurgitation of the aortic valve with a sub-valvular membrane. Given the symptoms and suspicion of endocarditis, he was initially treated empirically with vancomycin and piperacillin-tazobactam. He has an extensive history of chewing betel nuts and recently had routine dental cleaning.
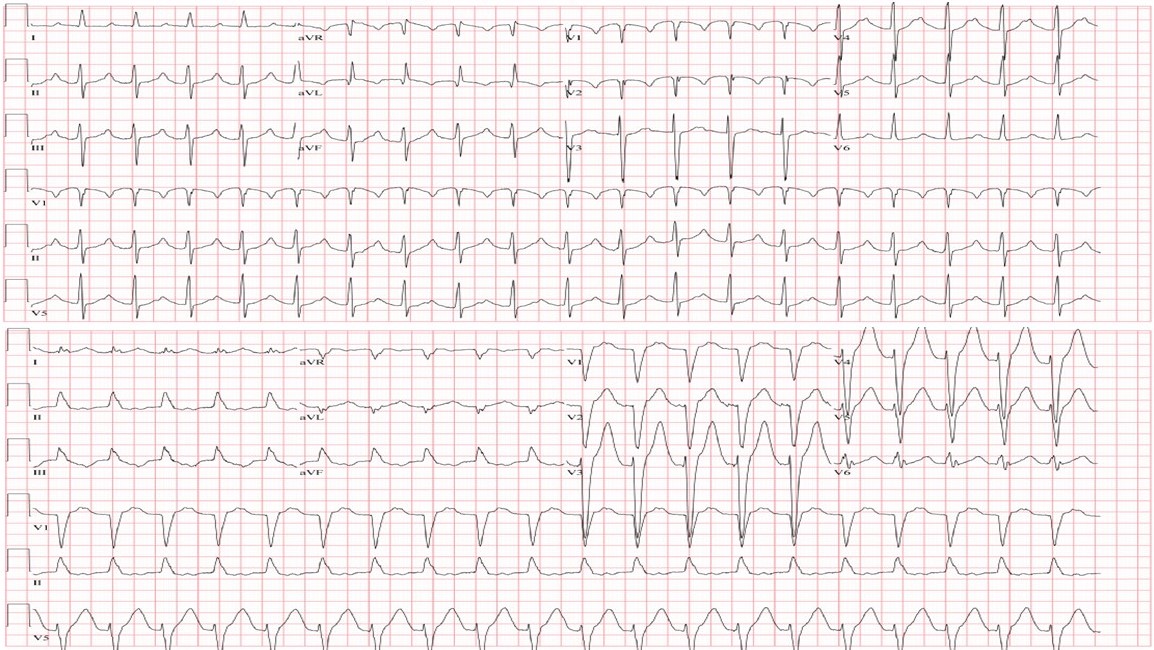
Initial laboratory results revealed a high white blood cell count of 15.9 x 10^9/L (normal range 4.8 - 10.8 x 10^9/L), high end of normal lactic acid at 1.6 mmol/L (normal range 0.5 - 2.0 mmol/L), an increased international normalized ratio of 8.0 (normal range 0.9 - 1.1), elevated lactate dehydrogenase at 627 IU/L (normal range 84 - 246 IU/L), haptoglobin levels of 162 mg/dL (normal range 62 - 197 mg/dL), and a procalcitonin level of 0.93 ng/mL (normal range <0.10 ng/mL). Blood cultures confirmed the presence of Aggregatibacter actinomycetemcomitans. Additionally, an electrocardiogram showed signs of conduction system involvement, including first-degree atrioventricular block and left bundle branch block, leading to the placement of a temporary screw-in pacemaker (Figure 1).
__progression_(bottom).jpg)
Further imaging with a transthoracic echocardiogram revealed excessive rocking motion of the 27 mm On-X mechanical aortic valve, suggesting valve dehiscence. A mobile mass measuring 5 mm x 7 mm was observed on the ventricular surface of the prosthesis, indicating a vegetation. Thickening of both mitral leaflets with a mobile echo density on the atrial surface of the posterior leaflet was also noted, suggesting another vegetation. A transesophageal echocardiogram confirmed the presence of three vegetations on the aortic valve, the largest measuring 10 mm x 19 mm, with extension into the posterior aortic root, indicative of an abscess and dehiscence (Figure 2). Blood cultures once again confirmed the presence of Aggregatibacter actinomycetemcomitans, leading to a switch in antimicrobial therapy to ceftriaxone for targeted treatment.

Due to the severity of the condition, the patient underwent emergent redo surgery, which involved debridement of the aortic abscess, insertion of a 21 mm On-X mechanical aortic valve (On-X Life Technologies, Austin, Texas, USA), and pericardial patch reconstruction of the aortic root. Following surgery, he received six weeks of intravenous ceftriaxone and experienced a successful recovery.
Discussion
Infective endocarditis is a relatively uncommon but significant cause of illness and death. Most infective endocarditis cases involve gram-positive bacteria, specifically staphylococci and streptococci, which account for approximately 80% of infections. Gram-negative organisms are responsible for about 10% of cases.1,2 HACEK endocarditis represents only 1-3% of cases, of which Aggregatibacter actinomycetemcomitans represents approximately 20% of HACEK endocarditis cases.1,3–5 Fortunately, the prognosis for HACEK endocarditis can be favorable if diagnosed promptly.
There is a notable difference in the occurrence of HACEK endocarditis between North America (0.3%) and the rest of the world (2%).2,3 Detecting HACEK endocarditis remains challenging, often leading to fatal outcomes.1 Typically, the condition progresses slowly, with patients experiencing nonspecific symptoms for an average of 13 weeks before diagnosis.1,3,4 These organisms are fastidious and require specialized culture media, exposure to carbon dioxide, and an extended incubation period for proper growth and identification.1,2,4 HACEK bacteria are commonly found in the oropharyngeal tract and can lead to periodontal infections, bacteremia, abscesses, and eventually endocarditis.1,4,5
Patients with HACEK endocarditis are generally younger, with a median age of 47, compared to 61 for non-HACEK endocarditis cases.1,2 Due to the subacute nature of HACEK infections, vegetations tend to be larger at the time of diagnosis compared to non-HACEK infections. HACEK infections also have a higher incidence of embolic events and vascular complications but are less likely to result in congestive heart failure.1 Aggregatibacter actinomycetemcomitans is responsible for approximately 20% of all HACEK endocarditis cases.1 These bacteria are part of the normal oropharyngeal microbiota and can breach the vascular barrier during routine oral hygiene procedures, mastication, dental infections, or dental procedures.1,2,4–6 Although considered low virulence, they tend to infect patients with prosthetic valves or underlying heart disease.1,4,6
Diagnosing Aggregatibacter actinomycetemcomitans HACEK endocarditis presents a challenge since these organisms do not easily grow on standard culture media.1,5–7 However, modern techniques, including automated blood culturing systems, have improved detection timeframes (median 3.4 days) comparable to other organisms.1,5–7 The Modified Duke Criteria are employed for diagnosis, requiring the presence of two major criteria, one major and three minor criteria, or five minor criteria to establish definitive endocarditis. In our patient’s case, he met two major criteria: 1) positive blood cultures for endocarditis, and 2) evidence of endocardial involvement with abscess, vegetation, and aortic valve dehiscence. Transthoracic echocardiogram, a non-invasive procedure, remains a reliable screening and diagnostic tool for infective endocarditis, with a specificity of up to 98%.1,7 In our patient, three large vegetations were observed on the aortic valve. If clinical suspicion remains high despite a negative transthoracic echocardiogram, a transesophageal echocardiogram should be performed.
The overall prognosis for HACEK endocarditis is generally more favorable compared to non-HACEK endocarditis.1–4 Antibiotic therapy is typically effective in treating HACEK endocarditis. However, urgent surgical intervention should be considered in cases with large vegetations, heart failure, extensive perivalvular involvement, persistently positive blood cultures, or prosthetic valve dehiscence.1,4 Penicillin was previously the antibiotic of choice, but due to the increase in beta-lactamase-producing HACEK organisms, first-line therapy now involves monotherapy with ceftriaxone, administered at a dose of 2 grams daily for approximately 4-6 weeks. Broad-spectrum fluoroquinolones can be an alternative for individuals with severe allergies to beta-lactams.1,5,6 In conclusion, though rare, HACEK endocarditis should be considered in patients with recent dental procedures and prosthetic valves. Culture negative endocarditis may be caused by recent antibiotic exposure; therefore, blood cultures should be obtained prior to antibiotic administration.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Jerry Fan
2401 S. 31st St
Division of Cardiology
Temple, Texas 76504
jerry.d.fan@gmail.com