INTRODUCTION
Rib fractures result in 248,000 emergency department visits and 48,000 hospital admissions annually in the United States.1 A National Inpatient Sample study revealed 373,053 rib fracture hospitalizations between 2007 and 2016, with 85% of patients presenting with multiple rib fractures.2 This study also indicated a significant increase in the financial burden of rib fracture hospitalization, rising from an estimated $209 million per annum in 2007 to $469 million per annum in 2016. One cohort study estimated a rib fracture incidence of 3.5 per 1,000 persons per year, with 24% of all non-spinal fractures being rib fractures.3 Up to 94% of rib fracture patients also have additional injuries with more than 50% requiring immediate surgery or admission to the Intensive Care Unit (ICU) level of care.4
The majority of rib fractures occur in older adults: patients who are 65 years of age or older.5 According to the United States (US) Census, there are 56 million adults over the age of 65 years, 16.8% of the total population.6 Hospitals in the US are now experiencing a higher volume of geriatrics patients and are faced with managing the health-related challenges this demographic brings. Older adults tend to be at heightened risk for respiratory complications following rib fractures such as pneumonia, acute respiratory distress syndrome, pulmonary embolism, pneumothorax, emphysema, and aspiration pneumonia.7 The mortality rate for rib fractures is substantial, approximately 10% for all ages.8 Although likely confounded by other concurrent traumatic injuries, such as head trauma, a retrospective study showed an increased mortality risk in patients older than 65.9 Each additional rib fracture in older adults compared to younger patients increases mortality by 19% and the risk of pneumonia by 27%.10 Data support a direct correlation between increasing numbers of rib fractures and increased pulmonary morbidity and mortality, with patients presenting with six or more rib fractures being at a higher risk for death from causes unrelated to the rib fracture.7 In the case of flail chest, which occurs when multiple ribs are broken in succession causing a paradoxical movement of the broken ribs, treatment in the intensive care unit (ICU) along with implementation of mechanical ventilation, chest tubes, epidural catheters, and/or surgical fixation is needed. A retrospective study on the National Trauma Data Bank found 82% of flail chest injuries required ICU admission.11 After adjusting for injury severity, comorbidities, and multiple rib fractures, patients 65 years and older have five times the odds of dying compared to younger age group.12 Patients sustaining blunt chest trauma and minor rib fractures should be admitted for close observation when presenting with subcutaneous emphysema because of possible delayed presentation of pneumothorax.13
Most rib fracture patients receive non-surgical management, and heal without significant complications. In the vulnerable geriatric population, this period of healing is crucial and requires additional multidisciplinary care. Lack of guidelines regarding the management of multiple rib fractures in older adults and concern for overuse of opiate pain medications by providers in this population led us to a scoping review of the evidence. We describe the most common causes of rib fractures, their management, the roles of various trauma and multidisciplinary team members involved in treating rib fractures (Table 1) and the utility of a multidisciplinary approach.
METHODS
Our review was drafted via the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) protocols. Articles included in this review focused on the causes, management, and existing protocols on rib fracture management. Peer-reviewed journal papers were included if they were published between the period of years 2000 – 2022, involved human participants and described management of rib fractures. Quantitative, qualitative, and mixed-method studies from PubMed and MEDLINE were included to consider different aspects of measuring treatment. Papers were excluded if they did not fit into the conceptual framework of the study.
RESULTS
A total of 57 articles were included in the scoping review. Information regarding rib fractures in older adults was organized in multiple categories. The first category was the causes and prevalence of rib fractures, followed by management of rib fractures. The third category was common causes for hospitalization and life-threatening complications, particularly in the presence of multiple rib fractures. Special attention was paid to pain management modalities and respiratory expansion techniques. Lasty, the utility of multidisciplinary approaches tailored to the needs and risks of geriatric patients and existing current protocols were reviewed.
A. CAUSES OF RIBS FRACTURE IN OLDER ADULTS
Blunt or penetrating trauma causes rib fractures. Two leading causes of these traumas in the older population are falls and motor vehicle accidents (MVA). Other mechanisms include gunshot injuries, pathological fractures, and stress fractures. A study that analyzed nearly 24,000 patients aged 65 years and older, between 2015-2016, reported the leading cause for rib fracture to be fall (67.6%) followed by transportation-related injuries (24.1%) and other or unspecified causes (8.3%).14
Falls
While most rib fractures in young adults result from high-energy trauma, the geriatric group tends to be more susceptible to rib fractures from minor traumas, such as a fall from a standing height.15 Low bone mass, slow gait speed, falling, impaired vision, and decreased muscle strength puts them at higher risk of falls.16 Osteoporosis, common in the geriatric age group, increases the risk of fracture. Up to 49 million people in 9 industrialized countries in North America, Europe, Japan, and Australia have met the World Health Organization’s criteria for osteoporosis.17
A cohort study found that low bone mineral density (BMD) at the femoral neck and lumbar spine was a strongly associated with rib fracture.18 Those with a rib fracture had a significantly lower femoral neck BMD. Men with a fracture had a BMD of 0.86 compared to a BMD of 0.94 for those without. The same trend was seen in women (Fracture: 0.84, Non-Fracture: 0.75).18 Low BMD and osteoporosis are common in women due to estrogen deficiencies after menopause.15
Prolonged use of glucocorticoids and cigarette smoking are some of the risk factors associated with bone loss and osteoporosis.16,19,20
Motor Vehicle Accidents
According to the Federal Highway Administration, licensed drivers aged 65 or older have increased dramatically since the year 2000.21 One study showed that older drivers, 70 years and above, have a higher fatality rate per 1,000 crashes compared to middle-aged drivers.22 A study conducted on the Crash Injury Research and Engineering Network (CIREN) database found that most rib fractures in the geriatric population are caused by impact with safety belts or airbags. Specifically, 92% of 211 patients aged 65 to 79 and 90.4% of 76 patients aged 80 and above had rib fractures.23 This may be due to age-related changes in vision, physical functioning, reasoning, and memory, as well as the impact of underlying diseases and medications altering older adults’ driving abilities.24 Adults older than 65 are at a higher risk of suffering traumatic injuries from MVAs.
B. MANAGEMENT OF ISOLATED RIBS FRACTURE
A crucial step in the management of isolated multiple rib fractures is deciding the necessity of hospitalization of the patient. The initial encounter and diagnosis of rib fractures often occur at primary care offices, urgent care centers, and emergency departments. Hospitalization is warranted in cases of rib fracture complications such as pneumothorax, hemothorax, lung contusion, flail chest, collapsed lung, and respiratory failure. Pain management coupled with pulmonary toilets using assistive devices has shown to reduce pulmonary complications.25,26 Surgical treatment can be indicated by more severe symptoms such as flail chest, chest wall deformity, and symptoms associated with nonunion.27
According to multiple studies, hospitalization is necessary for individuals sustaining multiple rib fractures.7,27,28 One study reported higher mortality associated with 3 or more posterior rib fractures.28 Flagel et. al. found that six or more rib fractures is a significant risk factor for death from causes unrelated to ribs fracture.7 The average age for surviving rib fracture patients was 47 years old, while the average age of non-surviving patients was 52. Mortality and other adverse effects increased when multiple ribs were broken. Mortality was 5.82% in patients with two rib fractures rising to 15.03% in patients with seven rib fractures. Fifty five percent of patients with five rib fractures had thoracic injuries which increased with each successive rib fracture. The incidence grew to 100% with eight or more rib fractures. A similar pattern was also seen in head injuries with a frequency of 40% of patients with five rib fractures having head injuries and up to 70% of patients with seven rib fractures. Complications such as pneumothorax, empyema, and aspiration pneumonia also showed a significantly increased incidence when the number of fractured ribs increased.
When observing geriatric patients, higher rates of pneumonia were seen with each additional rib fracture compared to younger patients.27 In 1-2 rib fractures, 18 % of older patients developed pneumonia compared to 2% of younger patients. The disparity increased further when looking at six fractures or more, where older adults had pneumonia incidence of 55% compared to 20% in younger patients. Since the force required to fracture multiple ribs is often enough to injure the upper torso, it may cause multiple associated complications, especially in the case of geriatric patients, necessitating transfer to a trauma center. Once hospitalized, the focus is on providing pain control and respiratory volume expansion strategies. Improved oxygenation and peak expiratory flow reflect the patient’s ability to take deep breaths and clear respiratory secretions.29
Rib Fracture Management
1. Pain management
Ineffective management of pain leads to decreased chest mobility and intercostal muscle spasm around the site of the fracture, which subsequently leads to decreased tidal volume and reduced cough. This exacerbates the risk of atelectasis in older adults in sitting positions for prolonged times, who are already predisposed to a reduced lung volume due to aging and any underlying chronic respiratory conditions such as asthma or chronic obstructive pulmonary disease.
A multimodal pain management approach is likely to address pain while minimizing side effects in the geriatric population (Table 2).30,31
-
Scheduled acetaminophen (oral or intravenous): acetaminophen has relatively fewer side effects and is better tolerated, however, the effect is modest.32
-
Opiates (oral or intravenous): should be minimized and started at the lowest effective dose. Balancing sedation is important as patient respiratory volume and status should not be compromised.
-
Topical medication: lidocaine patch can be a safe, effective adjunct for rib fracture pain.33
-
Insufficient pain management that does not relieve discomfort and/or concern for adverse effects including sedation or respiratory depression, the early involvement of the anesthesia team for regional nerve block, thoracic epidural, or paravertebral block may be beneficial. Trained emergency physicians can also conduct regional blocks including the serratus anterior block. Epidural analgesia has been shown to reduce pain in traumatic rib fractures when compared to intravenous analgesia, paravertebral block, and intercostal block.34 In the geriatric population, the risk of infection, prior spinal surgeries, and the use of anticoagulation/antiplatelet agents add an additional challenge to this mode of pain control. A multicenter cohort of injured older adults with multiple rib fractures reported up to 35% lower risk of delirium with regional anesthesia.35 Use of anesthetics without opiates is also beneficial in adults older than 65 by reducing/avoiding opiate-related adverse effects.36–38
-
Non-steroidal anti-inflammatory drugs (NSAIDs) should be reserved for case-by-case due to many potential side effects, including renal, cardiac and gastrointestinal (GI) toxicity. Geriatric patients are likely to have underlying comorbid conditions including GI or renal disease that limits the use of NSAIDs.39
2. Respiratory function/volume expansion strategies
In managing pulmonary complications of rib fractures, a comprehensive approach that encourages deep breathing, active coughing, and treatment of underlying pulmonary conditions is important. The utilization of assistive devices such as incentive spirometry (IS) and oscillatory airway clearance devices (OACD) can also play a crucial role in promoting lung function. These two devices help optimize breathing dynamics for patients.
A randomized controlled trial (RCT) in 2019 demonstrated IS reduced pulmonary complications and improved pulmonary function in patients with rib fractures.25 The American Association of Respiratory Care recommends this inspiratory maneuver, which involves maximal inspiration performed over five seconds followed by breath holding and normal exhalation.40 This can be challenging in geriatric patients due to conditions such as delirium and dementia, for whom OACD are an adjunct option that provides positive vibratory expiratory pressure treatment. An RCT compared IS with OACD after lung resection surgery and reported similar pulmonary function after surgery. OACD may be more comfortable for the patient to use.41
C. MULTIDISCIPLINARY APPROACH
Trauma nurses have been shown to have a critical role in documenting and tracking IS volume in patients with rib fractures, promoting early detection of respiratory decline.42 Early involvement of respiratory therapists, physical therapists, and occupational therapists has been associated with decreased ICU and hospital LOS.43 A systematic review showed acupuncture, transcutaneous electrical nerve stimulation (TENS), noninvasive ventilation (NIV) modalities, physiotherapy techniques, and multidisciplinary pathways used alongside pharmacological interventions are effective for use in the treatment of acute rib fractures.44 Grammatopoulou et al. investigated the effect of the active cycle of breathing technique (ACBT), added to standard physiotherapy management (body positioning, IS, supported coughing, and early mobilization), and analgesia administration on pain levels in adult patients with three or more rib fractures. This reduced pain on days 3-7 of hospitalization.45
In geriatric patients, the overall medical and cognitive status affects recovery and hospital LOS. Many of these patients are taking antiplatelet and anticoagulation agents, putting them at higher risk of developing hemothorax and subsequent need for chest tube drainage. Apart from pulmonary complications, these patients are also at a higher risk for delirium. The medical or geriatric team can help facilitate healing and recovery by adjusting medication, and preventing and managing delirium, medication-induced constipation, and GI bleeding (NSAIDs). Medical management of comorbidities such as hypertension, anemia, fluid overload, and diabetes needs concurrent management. Secondary fracture prevention strategies can be initiated during hospitalization. The involvement of a geriatrician in a trauma service to co-manage patients with multiple rib fractures has shown mortality benefits in patients greater than 80 years old.46 Superiorly located rib fractures represent more intense trauma to the chest and are associated with cardiac and great vessel injury whereas inferior ribs risk splenic and liver laceration which might require assistance from subspecialties including interventional radiology.47
Rib fractures take approximately 12 weeks to heal and patients typically regain up to 84% of their expected forced vital capacity, but it may be longer for older adults with underlying osteoporosis.48 Post hospitalization, a geriatric patient may require time in an acute rehabilitation or skilled nursing facility. At home they may require ongoing physical therapy and visiting nurse services. The involvement of a social worker and/or case manager may smoothen the transition of care.
Follow-up with the primary provider and/or a trauma surgeon is necessary to ensure healing and manage medications, especially in the case of chronic rib pain, persistence of pain after 3 months, which may disrupt daily function. Hearing, vision impairment also need to be addressed for recurrent fall prevention. In patients younger than 65 years, one study reported 9% of rib fracture patients were prescribed opioids on discharge but this number may greater in older adults due to limitations of other pain management options.49 Household measures include avoiding area rugs, and providing lighting, grab bars, handicap access, and assistive devices for safe ambulation. Home safety assessments can identify and address these issues.
On a community level, educating and enforcing road safety precautions such as seat belts, avoiding highways and unfamiliar roads, avoiding nighttime driving, driving sober, and undergoing a driving evaluation will likely help older patients stay safe and avoid traumatic injuries. Clear road signs, adults older than 65 cautionary crossing signs in suitable areas and illuminating lights in traffic signals/crossings are likely to help safe driving for older drivers who might have compromised visual acuity and neck movement-related disease. Education on smartphone taxi service apps may give older drivers an alternative method of transport.50
D. RIB FRACTURE PROTOCOL FOR OLDER ADULTS
Trauma centers, nationally, have shown better outcomes when rib fracture protocols were geared towards geriatric age groups. These protocols not only help to triage high-risk patients but also incorporate timely involvement of a multidisciplinary team. It is important to note that protocols can vary by center and can lead to different paths of management for similar cases. A study from North Carolina noted lower ICU admissions, fewer pulmonary complications, and shorter hospital lengths of stay (LOS) in a center with a rib fracture protocol.51 A level 1 trauma center in Rhode Island established a geriatric rib fracture protocol that resulted in decreased ICU LOS, mortality, and reduced need for mechanical ventilation.52 Multidisciplinary rib fracture protocol in a level 1 trauma center in Washington State incorporated early initiation of multimodal pain therapy, and frequent function-based scoring driven by nursing staff and the patient.53 The Western Trauma Association developed recommendations based on institutional practice and experience for rib fractures. They recommend admitting patients with more than 2 rib fractures and aged 65 or older to the ICU as well as patients with severe rib fractures, respiratory compromise, or patients who could not manage their pain.54
While hospital-based admission protocols help triage patients during initial encounters, providers face challenges regarding prognostication in geriatric age groups. Rib Fracture Frailty Index (RFF), which Choi et. al. reported to be a practical frailty risk stratification tool for geriatric patients with multiple rib fractures, may be helpful.55 When compared to three of the most popular scoring, a review noted that the Chest Trauma Score (CTS) was best suited to assess the risk in the geriatric population with a rib fracture, predicting poor outcomes within 24 hours of admission and thus likely requiring ICU admission.56 PIC (Pain, IS, and Cough ability) scores have shown to be a moderate discriminator of critical care need, and when PIC score delineation for ICU need appears to be at 7 or less; this threshold can be used during admission triage to guide care.57
DISCUSSION
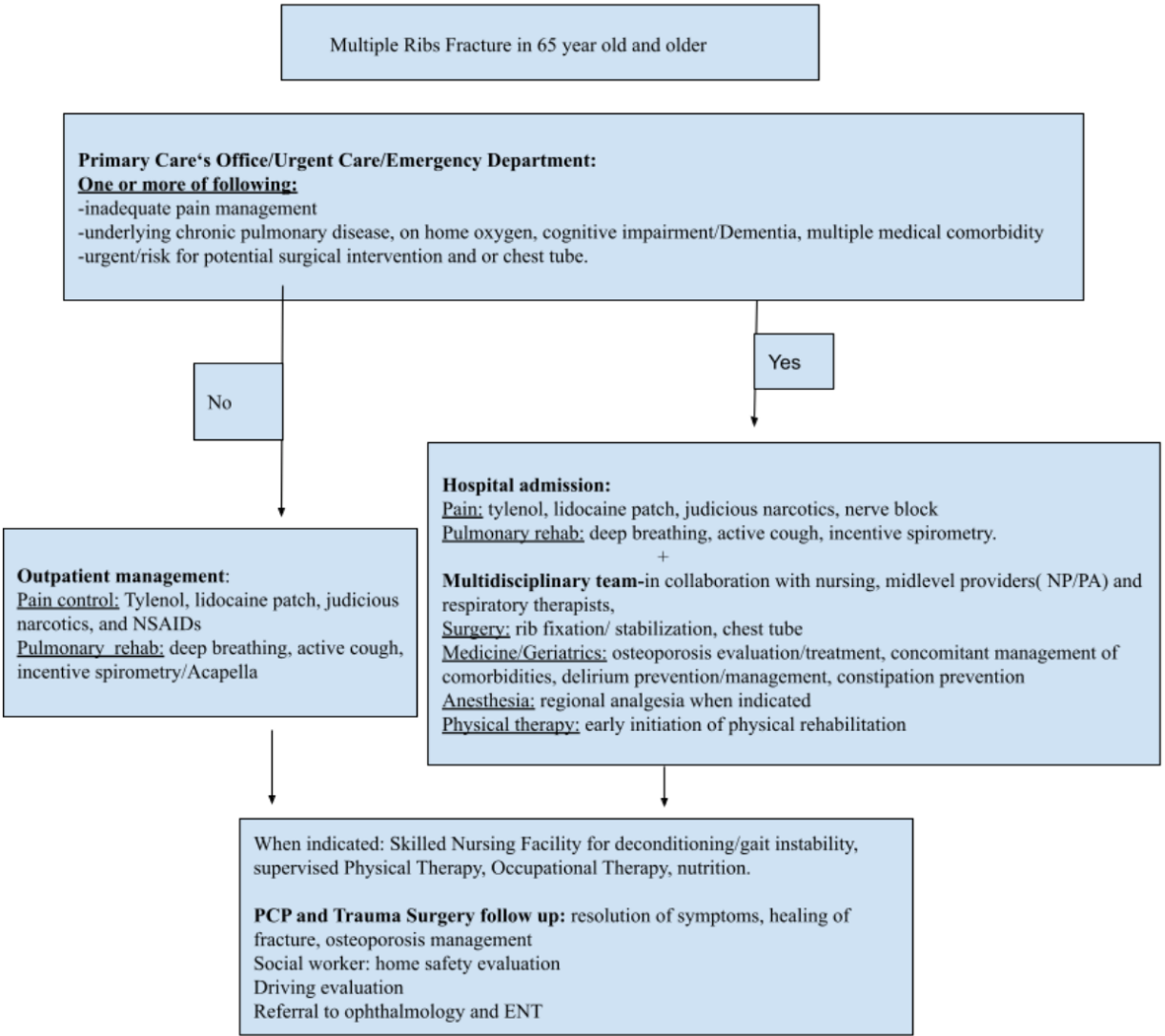
In this scoping review, we identified 57 papers published since the year 2000 regarding the complexity of management of multiple rib fractures. Older adults are at higher risk of rib fracture even with minor trauma and also at increased risk for complications. Although the number of isolated rib fractures gives a good guideline to the level of care, the location of the injury also deserves attention. Once triaged, a multidisciplinary team approach for rib fracture management can help to provide optimal care for patients. (Figure 1).

Our study has its limitations. We found that the mechanism of injury, the multimodal analgesia and protocol driven management were equally important. We noted that it remains a challenge to predict which patient might need more intense measures for pain management and who will require a chest tube. We also do not know to what extent frailty plays a role in the outcome of these older adults. The role of palliative care in severe trauma cases and very old patients is likely important but unclear.
In conclusion, we recommend an interdisciplinary team approach (Figure 1) in the management of multiple rib fractures. Randomized controlled trial is needed to explore the efficacy of collaborative protocol-driven management to develop guidelines for rib fracture in the geriatric population. Collaboration of outpatient providers, urgent care, and emergency department doctors who often see the patient for the first time, along with the trauma surgery team/ICU team, geriatric medicine, anesthesia, PT, and caregiver is of utmost importance to improve outcomes in older adults with rib fracture injuries.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Acknowledgments
None.
Corresponding Author
Iva Neupane, MD
Assistant Professor of Medicine
593 Eddy St
Providence, RI, USA
Email: iva_neupane@brown.edu