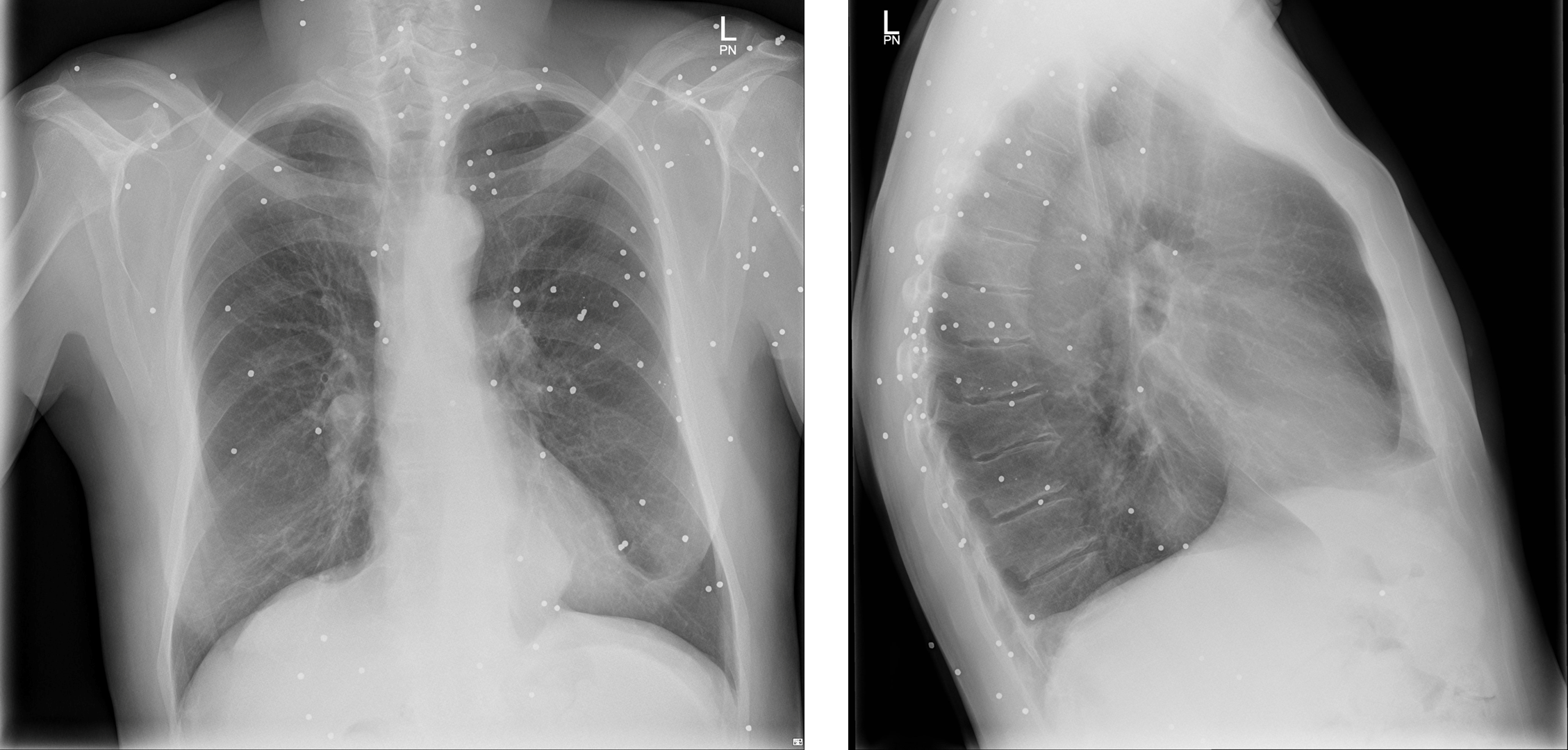
A man in his 70s with chronic obstructive pulmonary disease, opioid use disorder, and chronic untreated hepatitis C virus infection presented to the hospital with pancytopenia. His physical examination was notable for cachexia and his complete blood count revealed a white blood cell count of 2.74 (k/µL), hemoglobin of 8.4 (g/dL), and platelets of 47 (k/µL). As a part of an extensive work-up, a chest radiograph was obtained to evaluate for an occult malignancy. The radiograph revealed incidental findings of innumerable scattered, sub-centimeter metallic densities throughout the thorax and the subcutaneous tissue, consistent with retained bullet fragments from shotgun injury (Figure 1). The patient confirmed that he suffered a gunshot wound which had resulted in bilateral pneumothoraces over fifty years earlier. He denied any specific complaints related to the retained birdshot. The dispersion and clustering of the pellets seen on the lateral radiograph suggests that the patient was shot in the back, which was confirmed in review of his history.
_and_lateral_(right)_views_demonstrating_sc.png)
It is estimated that over 71,000 Americans are annually treated in emergency departments for nonfatal firearm injuries.1 Of these non-fatal injuries, nearly 90% of patients with nonfatal gunshot wounds will have retained bullet fragments which can lead to long-term consequences.2 Lead toxicity is a known life-threatening complication of retained bullet fragments if chelation is not initiated in patients with elevated lead levels.3 Fragments may also migrate to other tissues which can lead to damage of surrounding tissues. Additionally, patients with retained bullet fragments face challenges in obtaining magnetic resonance imaging as the ferromagnetism of the retained ballistic material is unknown.4
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Statement
No funding was obtained for this manuscript.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
None.
Corresponding Author
Tyler Larsen, MD, FACP
11301 Wilshire Blvd
Building 500, Suite 3214-B
Los Angeles, CA 90073
tlarsen@mednet.ucla.edu
310-478-3711 x47031