Background
The transition of care during hospital admission often necessitates adjustments to patients’ home medications, including oral hypoglycemics and anticoagulants.1 Direct factor Xa inhibitors have gained widespread use due to their efficacy, predictable pharmacokinetics, and ease of maintenance.2 However, during hospitalization, these agents may need to be switched to different forms of anticoagulation, such as unfractionated heparin (UFH) or low molecular weight heparin (LMWH). This switch may be required in cases of acute coronary syndrome, acute kidney injury, inability to tolerate oral medications, treatment failure, or surgical procedures.3,4
The transition from direct factor Xa inhibitors to UFH requires careful monitoring to ensure appropriate anticoagulation. Commonly used laboratory assays for monitoring UFH include the activated partial thromboplastin time (aPTT) and anti-Xa assays, with the latter becoming increasingly popular. Anti-Xa assays offer several advantages, including a more direct measure of heparin activity, a standardized reference range across all laboratories, and a higher proportion of tests within the therapeutic range compared to aPTT.5 However, direct factor Xa inhibitors can impact anti-Xa levels and potentially distort the accuracy of monitoring these levels, particularly during the initial stages of UFH initiation.6,7
Rivaroxaban and apixaban are direct inhibitors of human factor Xa, and their levels can be measured using liquid chromatography-mass spectrometry or commercially available anti-Xa chromogenic assays.8–12 Factor Xa levels are interpreted based on factors such as the type and dose of anticoagulant, as well as the time elapsed since the last administration. In certain clinical events, such as breakthrough thrombosis or bleeding, it may be necessary to assess relevant factor Xa concentrations and consider the use of additional assays, such as the activated partial thromboplastin time.13–15
This study aims to evaluate the safety of employing the standard anti-Xa assay protocol in patients who are receiving apixaban or rivaroxaban as maintenance therapy and subsequently switched to UFH during their hospital stay. The primary objective is to determine the incidence of adverse events, including minor bleeding, major bleeding, and thrombosis.
Methods
This is a retrospective chart review study that assesses possible bleeding or thrombotic events in patients who were started on UFH infusion during hospitalization following exposure to apixaban or rivaroxaban.
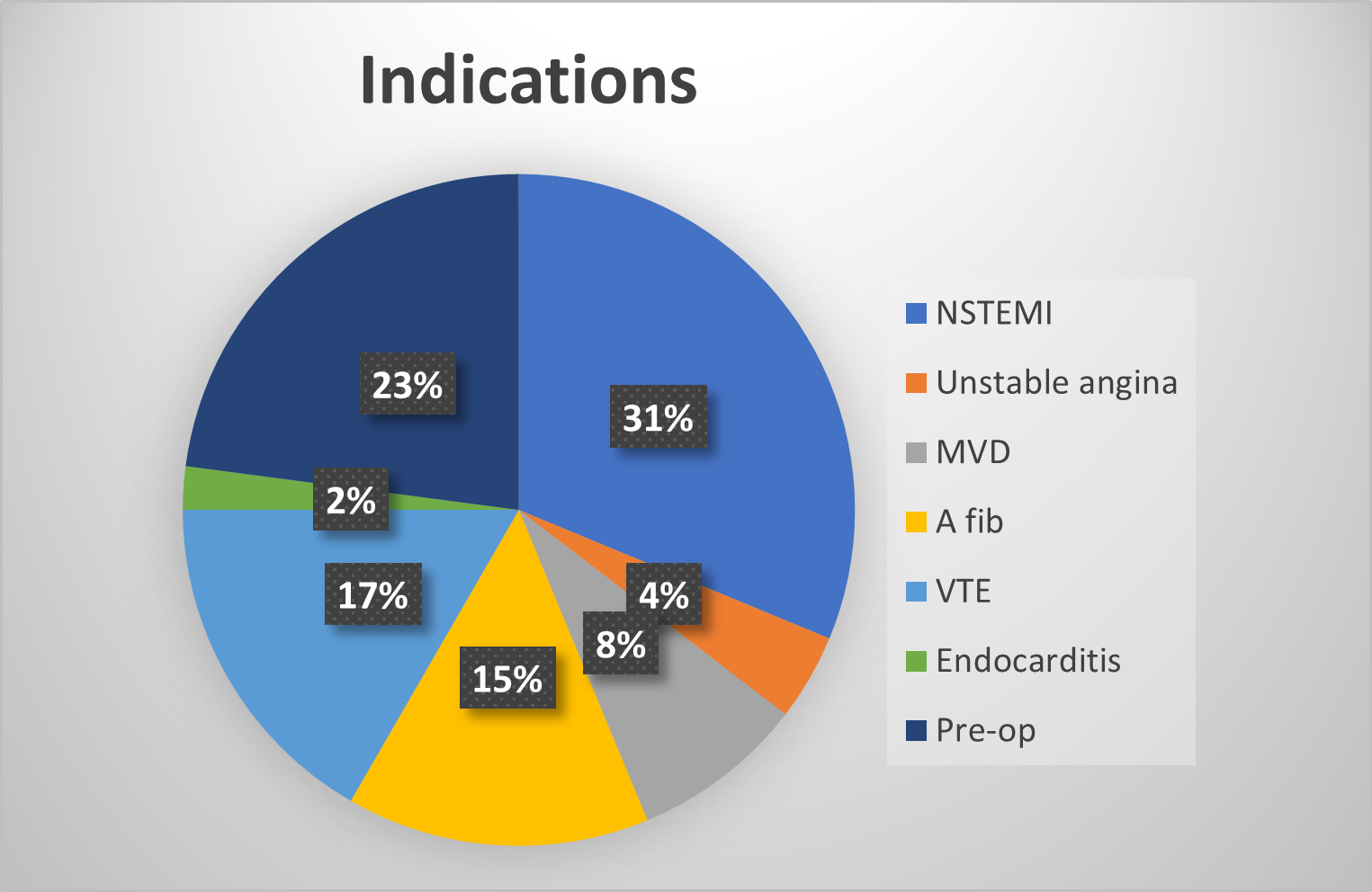
The study included patient records meeting the following criteria: any gender, any racial/ethnic background, age ≥18 and <90 years old, patients who were transitioned from apixaban or rivaroxaban to intravenous UFH at St. Vincent’s Medical Center (SVMC) in Bridgeport, CT, between December 1, 2020, and June 30, 2022, based on clinical indications. The indications included non-ST elevation myocardial infarction (NSTEMI), ST elevation myocardial infarction (STEMI), cerebrovascular accident, venous thromboembolic event (VTE), new-onset atrial fibrillation, or pre-operative procedure requiring bridging anticoagulation. Baseline anti-Xa plasma levels were recorded for all eligible patients. The therapeutic range for anti-Xa plasma levels in patients receiving UFH maintenance was set between 0.3 to 0.7 IU/mL.16 Patients less than 18 or more than 90 years old who were not using apixaban or rivaroxaban, and patients who only received a bolus of UFH or prophylactic heparin were excluded from the study.
The primary outcome of this study was to assess the incidence of adverse or serious adverse events. The analysis plan is descriptive in nature, focusing on evaluating the occurrence of events and examining sample characteristics. For continuous data, normality of distribution was assessed. Continuous data that exhibited a normal distribution were presented as mean and standard deviation. Categorical data were presented as frequency and percentages. An alpha (α) value of 0.05 was used to determine statistical significance. All analyses were performed using Excel 2021.
Results
A total of 48 patients were included in this study. The average age of the patients was 70.52 years. Females accounted for 40% of the study population, while males constituted 60%. The majority of the study participants were white. Among the patients, a higher proportion (83%) were maintained on apixaban compared to rivaroxaban (17%). The indications for transitioning to intravenous unfractionated heparin are displayed in Figure 1. The average time from admission to the initiation of intravenous UFH was 31 hours, and the average duration of UFH use during hospitalization was 61 hours.

A total of 13 patients experienced bleeding or thrombotic complications, with 12 cases (25%) involving bleeding and one case (2%) involving thrombosis, specifically a myocardial infarction. Half of the bleeding events were gastrointestinal (GI) bleeds, while 33.3% were soft tissue bleeds, and 16.67% were genitourinary (GU) bleeds. GI bleeds encompassed upper or lower GI bleeding, while GU bleeds included cases of hematuria. Soft tissue bleeds referred to intracompartment bleeds, such as retroperitoneal hemorrhage. Among the patients who experienced complications, 57% had baseline anti-Xa levels above the therapeutic range for UFH. The mean baseline anti-Xa level was 0.92 U/mL. There was no statistically significant difference in baseline anti-Xa levels between patients with complications and those without complications (p-value 0.26).
Discussion
Coagulation refers to a complex system that maintains the fluidity of the blood in the vascular system while allowing for the rapid formation of a solid blood clot to prevent hemorrhaging subsequent to blood vessel injury. Such system is composed of numerous vessel walls, platelets, coagulation factors, inhibitors, and the fibrinolytic systems.17 Several techniques, including clot-based tests, chromogenic or color assays, direct chemical measurements, and ELISAs, are used for coagulation testing.18 The activating partial thromboplastin time (aPTT) allows measurement of optimal activation of contact factors (factor XII, factor XI, prekallikrein, and high-molecular-weight kininogen).19 Low-molecular weight heparin (LMWH) usually forms an inhibitory complex with antithrombin to inactivate activated factor X (Xa). An anti-factor Xa assay quantitatively measures the pharmacodynamic effect of the inhibition of factor Xa by LMWH.20
One of the benefits of anti-Xa assays is to prevent over- or under- anticoagulation which can lead to potential negative outcomes.21 Despite the titration of UFH infusions guided by anti-Xa levels, adverse outcomes can still occur, as observed in this study. Although the baseline difference in anti-Xa levels was not statistically significant between patients experiencing adverse thrombotic/bleeding events and those without adverse events, the mean anti-Xa level was higher in patients with bleeding outcomes. This finding may suggest the need to initiate UFH infusions at a lower rate than usual or to delay UFH initiation until adequate clearance of direct factor Xa inhibitors is achieved in cases involving recent use.
Since direct factor Xa inhibitors can lead to supratherapeutic anti-Xa levels,21,22 bleeding episodes may be expected. The incidence of bleeding events in patients with supratherapeutic anti-Xa levels in the context of recent direct factor Xa inhibitor use is estimated to be 3% for major bleeding events and 3% for non-major bleeding events.22 However, the frequency was higher in our study. The majority of our patients underwent UFH infusion for acute thrombotic events, including NSTEMI and VTE. Studies have demonstrated a lower rate of VTE recurrence when the target therapeutic anticoagulation values are attained within 24 hours after the initiation of UFH infusion.23 Therefore, a previous use of a direct factor Xa inhibitor, which affects baseline anti-Xa, may be a risk factor for thrombotic recurrence.
There is conflicting data regarding whether prior use of direct factor Xa inhibitors can increase the rate of in-hospital bleeding events. For instance, in patients admitted for STEMI, the use of home direct factor Xa inhibitors was not found to be associated with an increased incidence of in-hospital major bleeding.24 On the contrary, intracranial bleeds were significantly increased among admitted patients maintained on apixaban or rivaroxaban at home, according to another study.25 Risk factors for bleeding included age greater than 80 years, inappropriately high dosing regimens, and modest anti-Xa levels.25
Activated partial thromboplastin time (aPTT) assays can also be used to monitor and titrate heparin dosing, as was historically the case prior to the year 2000.26 However, it is interesting to note that aPTT levels have been found to be more strongly associated with an increased incidence of bleeding than anti-Xa levels,26 particularly in the pediatric population. Conversely, there was no significant difference in clinical outcomes between anti-Xa and aPTT-based monitoring of unfractionated heparin (UFH) infusion.27 Direct factor Xa inhibitors might affect aPTT, but aPTT can often still be normal in these cases.28
There are several limitations to our study. Firstly, being a retrospective chart review study, it is challenging to eliminate potential confounding factors, as the data relies on existing medical records. Secondly, the diagnosis of bleeding or thrombosis was determined based on chart documentation, which is subject to potential variations in accuracy and completeness of the recorded information. Additionally, it is unclear whether bleeding events had already commenced prior to the initiation of UFH infusion, which could impact the interpretation of causality. Thirdly, the specific time elapsed since the last intake of apixaban, or rivaroxaban was not available, leading to inclusion of patients based solely on self-reporting of their use of these medications. Lastly, it is worth noting that normal anti-Xa levels observed in some cases may be attributable to medication errors or limitations in medication adherence.
Conclusion
Patients who are on direct factor Xa inhibitors as part of their home medication regimen may require bridging to unfractionated heparin (UFH) when they are admitted to the hospital. This bridging is often necessary for various reasons, including myocardial infarction or venous thromboembolic events. Monitoring the bridging process is crucial, and anti-Xa assays are available to assess the extent of anticoagulation. However, it should be noted that the use of apixaban and rivaroxaban, which are direct factor Xa inhibitors, can potentially impact anti-Xa levels, increasing the risk of bleeding or thrombotic events. Therefore, it is essential to establish baseline anti-Xa levels to guide the subsequent use of UFH or determine the suitability of alternative assays, such as the activated partial thromboplastin time (aPTT).
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Georges El Hasbani MD
Department of Internal Medicine
St. Vincent’s Medical Center
Bridgeport, CT 06606
Email: george.hasbany@lau.edu