Background
The most common causes of acute pancreatitis are biliary lithiasis (40%) alcohol consumption (30%) and hypertriglyceridemia. Other less common causes are idiopathic, hereditary, drug-induced, iatrogenic, infectious, hypercalcemia, autoimmune, trauma, pregnancy, or ischemia.1–3 In patients with primary hyperparathyroidism, acute pancreatitis is reported in 3-15%. The association with hypercalcemia is believed to be due to raised intracellular calcium that activates calcineurin, leading to intracellular activation of pancreatic enzymes such as trypsin and activation of NF-kb (nuclear factor kappa-light-chain-enhancer of activated B cells) and consequent pancreatic damage.3,4 It has also been associated with calcium deposition in the pancreatic duct with consequent obstruction.3 We describe a young woman who presented with acute pancreatitis, and found to have hyperparathyroidism secondary to a parathyroid adenoma.
Case Presentation
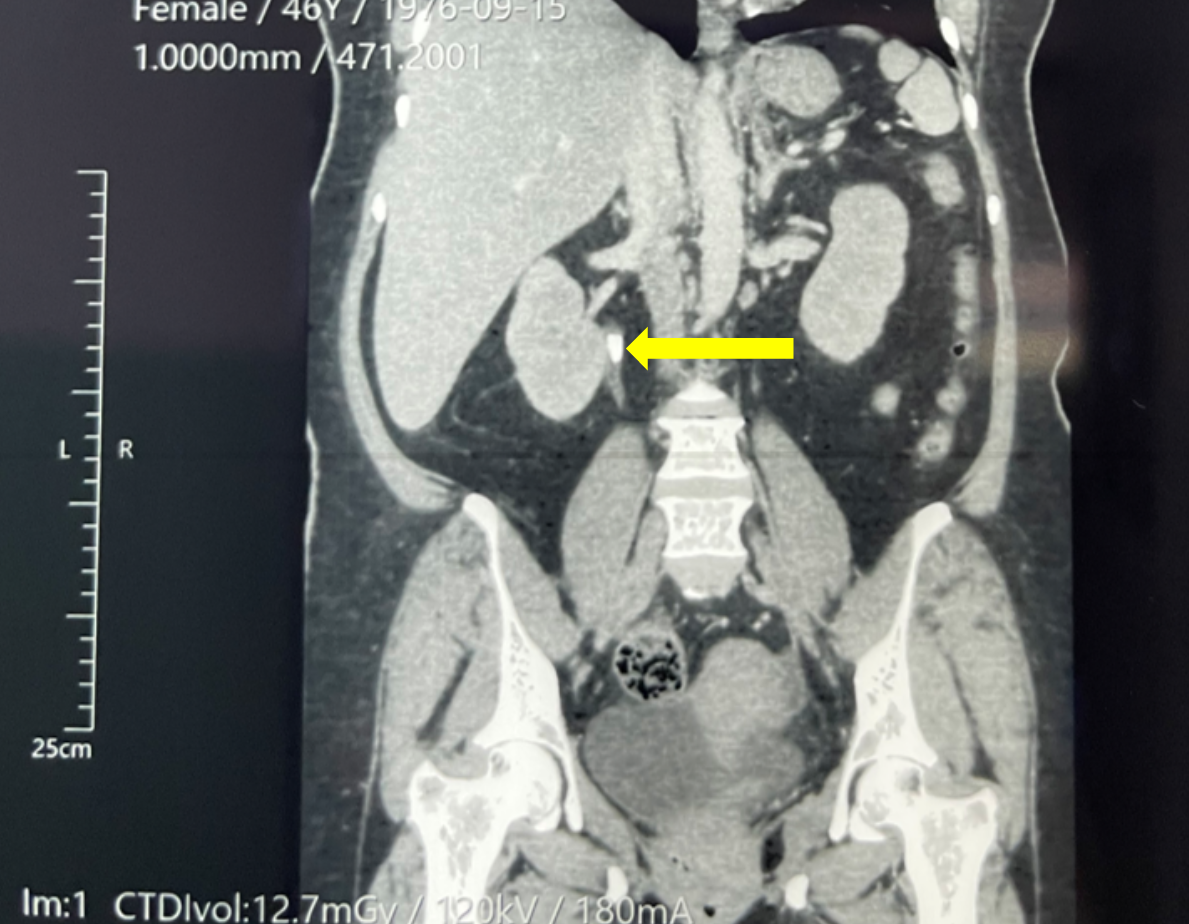
A 46-year-old woman with a past medical history of type 2 Diabetes Mellitus treated with metformin presented with three days of abdominal pain radiating towards the back. The pain was partially relieved by bending forward and aggravated with food. Several episodes of nausea and vomiting accompanied the pain. On physical examination, there was tenderness to palpation in the epigastric area. Her laboratory values at the time of presentation are described in Table 1. Her amylase (245 u/L) and lipase (236.6 u/L) were elevated among those. Her arterial blood gases with pH 7.42, Pc02 34.6 mmHg, p02 77.6 mmHg, bicarbonate 22.1 mmol/L. BISAP score was 1. She was treated with intravenous fluids and analgesics. A computerized tomography (CT) scan of the abdomen and pelvis with contrast revealed bilateral renal microlithiasis, right hydroureteronephrosis secondary to calculus in the renal pelvis (Figure 1), Balthazar C pancreatitis (inflammatory changes in pancreas and peripancreatic fat) and left adnexal cyst.
.png)
Given the CT findings, a parathyroid hormone (PTH) level and calcium levels were obtained. The PTH level was 240.20 pg/ml (reference 14.90 – 56.90 pg/ml), and serum calcium was 14mg/dl. A neck ultrasound revealed a right parathyroid adenoma. She was treated with aggressive intravenous fluids, loop diuretics, corticosteroids, and bisphosphonates. There were no acute EKG changes. Despite these measures, her PTH levels were elevated at 466.70 pg/ml and serum calcium at 14.84 mg/dL. Urinary calcium was noted to be 369.60 mg. Given the lack of improvement, she was transferred to the oncologic surgical service, and a parathyroidectomy was done ten days after her initial presentation. The biopsy showed findings compatible with parathyroid adenoma in the right parathyroid gland. She was discharged home following the surgery.
Discussion
Acute pancreatitis is a disease that is characterized by damage to the acinar cells and the release of trypsinogen within the acini, which is activated and promotes direct injury to the pancreas. It has an incidence of 110-140 per 100,000 population. The diagnosis is made with 2 of 3 criteria: abdominal pain with clinical characteristics of pancreatitis, serum amylase or lipase elevation greater than three times the upper limit of normal, and imaging suggestive of acute pancreatitis.5 In this case, the patient had 2 of 3 criteria present. Computed tomography during the first day of hospitalization was made because of the high suspicion of acute pancreatitis with enzymes not elevated three times the upper limit of normal and to rule out other complications of hypercalcemia (nephrolithiasis).
Primary hyperparathyroidism is a disorder in the function of the parathyroid gland characterized by hypercalcemia and elevated parathyroid hormone.1 It is the product of the autonomous production of one or more abnormal parathyroid glands. A small percentage of patients are normocalcemic. Most cases are sporadic; however, other causes, such as previous radiation exposure, radioactive iodine therapy, medications (thiazides, lithium), or genetic disorders, have been associated.2 The number of glands involved is variable. The presenting forms of the disease are adenoma (80-85%), glandular hyperplasia (5-15%) or carcinoma (1%). Severe hypercalcemia (greater than 15 mg/dL), parathyroid hormone values greater than 500 pg/ml, and age over 70 are predictors of parathyroid cancer. The most common complication is nephrolithiasis, affecting 15-20% of patients. Among the gastrointestinal complications are constipation, epigastralgia, and hyporexia. It can also manifest as easy fatigability, weakness, lethargy, depressed mood, psychosis, cognitive dysfunction, hypertension, arrhythmias, or valvular calcification. The incidence of acute pancreatitis ranges from 1-10%.2
Primary hyperparathyroidism (HPTP) is the leading cause of hypercalcemia in the hospital setting and has an incidence of 1-2 cases/1,000 admissions. The biochemical and clinical manifestations of HPTP are related to the increase of parathyroid hormone with hypercalcemia.6 Hypercalcemia secondary to primary hyperparathyroidism is a rare cause of acute pancreatitis. Although the pathophysiological mechanism is unclear, hypercalcemia is considered to activate the intrapancreatic conversion of trypsinogen to trypsin, leading to pancreatic damage.3 It has also been associated with calcium deposition in the pancreatic duct with consequent obstruction.2
In recent years, attention has been paid to the existence of a genetic substrate. Mutations in the SPINK1 (serine protease inhibitor Kazal type I) and CFTR (cystic fibrosis transmembrane conductance regulator) genes have been detected in patients with HPTP who developed acute pancreatitis. Mutations in the CTRC gene (chymotrypsin C) have also been found.7 SPINK1 is a specific trypsin inhibitor, the mutated variant of which has a decreased ability to inhibit trypsin, which can be prematurely activated in the pancreas. The CASR gene (calcium receptor gene) has also been implicated, although its role in this process is unclear. These are genes involved in regulating lysosomal membrane permeability, intracellular calcium homeostasis, and controlling trypsin activation.7,8 In Central America, no genetic tests are available to diagnose mutations in acute pancreatitis and hyperparathyroidism association.
Patients with primary hyperparathyroidism and hypercalcemia have ten times the risk of pancreatitis than the rest of the population. However, it occurs in only 1-10% of patients with primary hyperparathyroidism. The prevalence of primary hyperparathyroidism is 1-7 per 1000 adults.1 Single adenoma is the most frequent cause of primary hyperparathyroidism, as in the patient’s case, in which a mass was not evident or palpable at the cervical level, finding evidence of it by ultrasound.2 The best therapeutic option for primary hyperparathyroidism in our patient is surgical resection of the parathyroid gland.3 In conclusion, hypercalcemia can induce pancreatic damage by pathologically activating intrapancreatic trypsin. It is suspected that pancreatitis is also the result of additional genetic and environmental influences. Because of this and the incidence of association between pancreatitis and hyperparathyroidism is very low, it is recommended to exclude secondary causes of pancreatitis.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest