Background
Meckel’s diverticulum (MD) is caused by the partial obliteration of the vitelline ducts. It is frequently described using the rule of 2s: 2% of the population, within 2 feet of the ileocecal valve, 2 types of heterotopic mucosa, 2-inch-long, and presentation before the age of 2. In children, gastrointestinal bleeding is the typical presenting symptom of MD, whereas, in adults, obstruction brought on by intussusception or adhesive bands are the usual presenting symptoms.1,2 Perforation is a rare presentation in both populations.
Perforated MD presents with symptoms including fever, chills, nausea, vomiting, right lower quadrant abdominal pain, and peritoneal signs, which resemble symptoms of acute appendicitis. This resemblance frequently leads to inaccurate diagnostic results. Even though adult symptomatic MD is rare, it is still associated with significant morbidity. We present the case of an otherwise healthy 49-year-old male who presented with signs and symptoms of peritonitis, and was eventually diagnosed with a gangrenous and perforated MD.
Case Presentation
A 49-year-old male with no significant past medical history presented with spasmodic abdominal pain, worsening abdominal distension and multiple episodes of bilious vomiting. He denied passing gas or having bowel movements. He smoked regularly and did not take any medications at home. At the time of presentation, he had a blood pressure of 96/72 mmHg, a heart rate of 126/min, and he was afebrile. On exam, the abdomen was distended, with diffuse tenderness and guarding. There was no palpable mass or free fluid. Bowel sounds were absent on auscultation. He was admitted to the medical service and started on intravenous fluids. A Ryle’s tube was inserted, and bowel rest was maintained. A CT scan of the abdomen and pelvis was done, and broad-spectrum antibiotics were started intravenously.
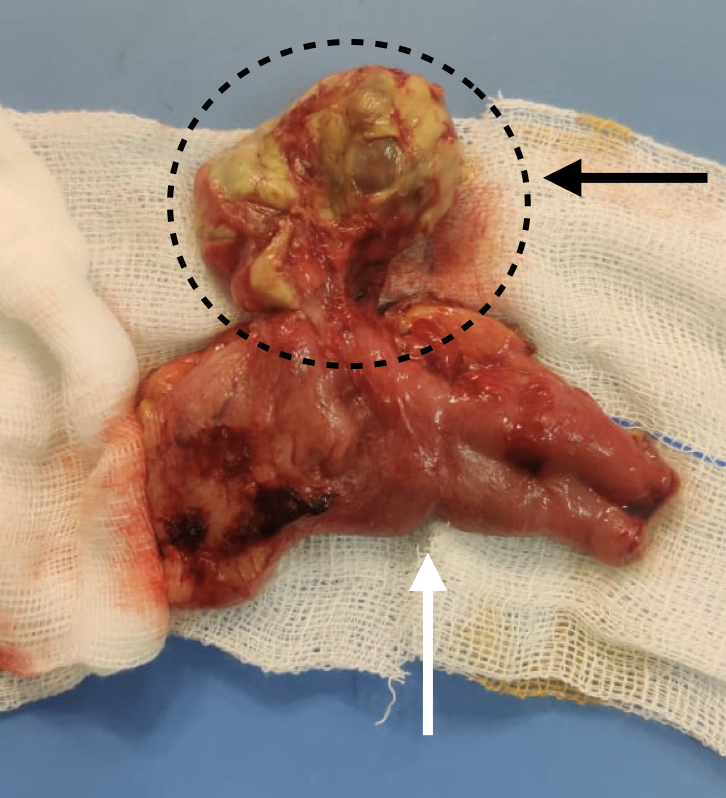
The CT scan demonstrated multiple grossly dilated bowel loops with air fluid levels and mild free fluid. The transition zone was noted at the terminal ileum. The presumed diagnosis was sub-acute intestinal obstruction, and the patient was taken to the operating room (OR) for an exploratory laparotomy. There were grossly distended small bowel loops in the OR, and a gangrenous and perforated MD was present 20cm proximal to the ileocecal junction. The MD was resected along with the adjacent bowel, and a side-to-end anastomosis was done. Biopsy of the resected segment was suggestive of MD with inflamed and necrotic mucosa (Figure 1).
_along_with_segment_of_ileum_(white_arrow).png)
The patient’s Ryle’s Tube was removed on postoperative day (POD) three. He underwent postoperative bowel rest for three days and was allowed to eat on POD four. However, the patient developed postoperative ileus, which was managed conservatively with re-insertion of the Ryle’s Tube and the use of pro-kinetic drugs. A postoperative CT showed mild inter-bowel collection. On POD 7, the patient was allowed to eat again after clamping Ryle’s tube. The Ryle’s tube and drain were eventually removed on POD 8. At discharge, he was able to pass flatus and faeces and showed a good tolerance for oral consumption.
Discussion
The dysgenesis of the small bowel, as it develops in relation to the embryological yolk sack, leads to MD. It develops due to the vitelline duct’s incomplete obliteration between the fifth and eighth weeks of pregnancy. Therefore, MD is a real diverticulum with a separate blood supply. Up to 60% of symptomatic cases have ectopic tissue, with gastric mucosa being the most frequently found type.3 The most frequent congenital gastrointestinal malformation, MD, only affects 2–4% of the general population. The most common age of presentation for symptomatic MD, which presents as gastrointestinal bleeding, is ten years old.4 Even less frequently occur symptomatic MD in adults. From 4.4% to 6.4% is the estimated lifetime risk for developing MD complications.5,6 Bowel obstruction is the most typical adult presenting symptom, followed by GI bleed and diverticulitis.1,2
Because the differential diagnosis is broad and the presenting symptoms can be non-specific, the preoperative diagnosis of a patient with MD frequently poses a challenge to the clinician in both children and adults.7 Haemorrhage, bowel obstruction, inflammation, perforation, intussusception, volvulus, and malignant transformation are complications of MD.8 Meckel’s scans, also referred to as radionuclide scans, are a promising imaging technique for identifying MD. However, the paediatric population seems to be the target audience for this strategy. When used in paediatric patients, scintigraphy has an accuracy rate of over 90%, but when used in adults, this accuracy rate drops to approximately 46%.9 Less than 10% of MD cases in adults are diagnosed before surgery because of the radionuclide scans’ decreased accuracy and the diagnostic difficulties. Most MD cases in adults are discovered during surgical procedures.
Complications in adulthood are rare among individuals with MD, and most of them live without any symptoms.10 MD perforation can mimic acute appendicitis and manifest as an acute abdomen.11 In addition, MD can rupture spontaneously due to progressive inflammation of the diverticulum wall, as in our case, which led to peritonitis, or it can rupture due to a foreign body due to irritation of the foreign body and pressure necrosis of the diverticulum wall.12 Given the resemblance in clinical and imaging features with various other acute surgical and inflammatory abdominal conditions, diagnosing a complicated Meckel’s diverticulum before surgery can be challenging. Nevertheless, securing an accurate diagnosis increases the probability of utilizing a laparoscopic approach for its treatment.13 Complications arising from MD are infrequent and can be challenging to detect. Achieving the best outcomes for such patients hinges on early diagnosis and swift surgical intervention.
For asymptomatic Meckel’s diverticulum cases, the data is presently inconclusive, and treatment decisions are at the discretion of the physician. A risk score is suggested by one study based on the following four risk factors: male sex, patients under the age of 45, diverticula longer than 2 cm, and fibrous bands. If the risk score is greater than or equal to 6, resection can be done on an asymptomatic patient. Surgery is not typically performed when asymptomatic patients receive an incidental imaging diagnosis; however, the criteria for surgery for asymptomatic patients are still debatable.14 In conclusion, acute abdominal pain is a common symptom of spontaneously perforated MD, which is challenging to diagnose before surgery. Perforated MD should be considered as a differential diagnosis, even for adult patients who experience sudden abdominal pain that mimics acute appendicitis.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors have no conflict in interest to disclose.
Corresponding Author
Riecha Joshi
Department of Pediatrics,
Government Medical College, Kota, India
Email: riechajoshi08@gmail.com
Phone: +17043187926