Background
The post-acute sequelae of COVID-19 present in myriad ways and can affect multiple organ systems. The hypothalamus performs various functions, including temperature regulation and control of the autonomic nervous system. Cluster headache belongs to a group of trigeminal autonomic cephalgia’s with pathophysiology implicating the role of the hypothalamus in its origin. We present a young girl with fever of unknown origin (FUO) and a secondary cluster headache likely related to SARS-CoV2.
Case Presentation
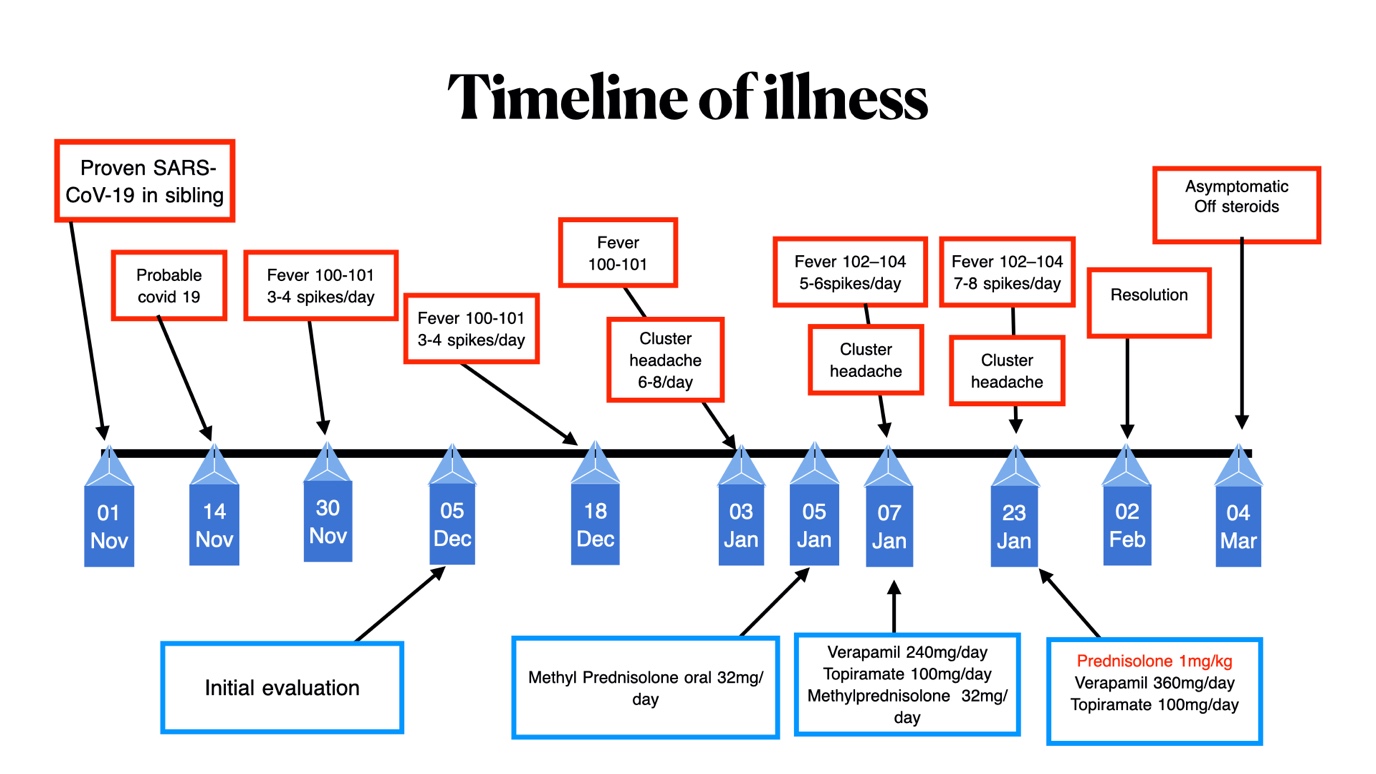
A 17-year-old girl with no significant past medical history presented with intermittent febrile episodes, each lasting from 30 minutes to one hour, relieved by acetaminophen. The patient was asymptomatic between the episodes without any constitutional or organ-specific symptoms. Over two weeks, an extensive workup in the hospital yielded no positive findings, meeting Fever of Unknown Origin (FUO) criteria. One month following her initial presentation, she developed unilateral severe right-sided headaches, 6-8 daily episodes lasting 30-45 minutes with ipsilateral conjunctival congestion, lacrimation, and eyelid edema with a sense of restlessness, classified as cluster headache per ICHD-3 criteria.1 Her 13-year-old sibling was on treatment for granulomatosis with polyangiitis over the last four years. On further probing, two weeks before the onset of the current syndrome, she had a high-risk exposure to her sibling, who had been infected with SARS-CoV-2. One week after the exposure, she developed upper respiratory tract symptoms and a fever ten days later. As respiratory symptoms were very mild, she had not undergone testing for COVID-19 at the onset. Upon admission for FUO workup, SARS-CoV-2 reverse transcriptase polymerase chain reaction was negative. Serological workup for infectious causes and inflammatory/connective tissue disorders was negative.
A whole-body positron emission tomography (PET) scan showed minimal uptake in the left knee joint. Magnetic resonance imaging scan of the brain with contrast and cerebrospinal fluid studies, were normal. Because of the history of high-risk exposure with the development of respiratory symptoms one week later, the possibility of a SARS-CoV-2-induced hyperinflammatory response was considered; however, all the inflammatory markers, including interleukin-6, were negative. Considering the duration of her illness, she underwent SARS-CoV-2 IgG testing, which was elevated. Figure 1 provides an approximate timeline of the patient’s illness.

Despite a comprehensive workup, no infectious, inflammatory, or neoplastic cause could be identified to account for her FUO and the development of a cluster headache. Hence, despite normal inflammatory markers, the possibility of a probable delayed inflammatory response to the SARS-CoV-2 antigenic trigger was considered, and she was initiated on oral steroids (methylprednisolone 32 mg per day). Her headaches did not exhibit any improvement with the medications, which included daily oral methylprednisolone at a dosage of 32mg, verapamil at 360mg per day, and topiramate at 100mg per day. Consequently, the steroid dose was escalated to 1mg/kg of prednisolone. Over the next week, her fever spikes reduced, and her headache eventually resolved. She was discharged on oral corticosteroids, which were tapered and discontinued. The patient was asymptomatic at the last follow-up visit.
Discussion
Despite being a multi-system disorder with myriad presentations, SARS-CoV-2 infection presenting as trigeminal autonomic cephalgia is infrequent. The pathophysiology of cluster headaches may be understood through the mechanism in which the SARS-CoV-2 virus enters the trigeminal ganglia via branches of the trigeminal nerve, leading to the release of substance P and calcitonin gene-related peptide (CGRP), both of which are implicated in the inflammation and nociception processes.2 At the receptor level, binding of SARS-CoV-2 leads to internalization of angiotensin converting enzyme-2(ACE-2); a transmembrane metalloproteinase, reducing its activity. The vascular endothelium has an abundance of ACE-2, which acts in conjunction to activate the trigemino-vascular system. Neuroinflammation resulting from pro-inflammatory cytokines such as interleukin-1 beta and NF-κB secondary to SARS-CoV-2 could play an additional role in triggering inflammation. The hypothalamus is functionally connected to the trigemino-vascular system and plays a role in the generation of cluster headache by stimulating the insula, frontal cortex, and cingulate cortices. The inferior posterior hypothalamic grey matter plays a major role in generating cluster headaches.1 CGRP has been postulated to be a mediator in the genesis of cluster headache. During an episode of cluster headache, the release of vasodilatory molecules such as CGRP, vasoactive intestinal peptide activates the trigemino-parasympathetic system, leading to vasodilation and autonomic manifestations.3
The hypothalamus acts as a temperature regulator, and local prostaglandin E plays a crucial role in neutrally mediated thermogenesis, along with an imbalance between inhibitory and excitatory sympathetic pathways.4 The activation of the trigemino-vascular system by SARS-CoV-2 may cause release of cytokines and neuromodulators from the trigeminal ganglia, activating the thalamus. Localized inflammation in the hypothalamic area might serve as the underlying trigger for her clinical symptoms. Isolated hypophysitis could potentially explain the clinical manifestations without a simultaneous increase in serum inflammatory markers. Our comprehensive evaluation of the patient, characterized by the absence of evidence for systemic inflammation, provides further credence to this hypothesis.
Granulomatosis with polyangiitis (GPA) predisposes first-degree relatives to other autoimmune disorders owing to genetic susceptibility, such as systemic lupus erythematosus and Sjogren’s syndrome.5 The diagnosis of GPA in younger siblings could suggest a pro-inflammatory milieu in our patient. It is likely that our patient experienced a mild COVID-19 infection, and her acute post-COVID sequelae manifested as FUO. The occurrence of simultaneous febrile episodes with a relatively symptom-free period in between, coupled with the emergence of secondary cluster headaches, may point to a common underlying mechanism affecting the hypothalamus. Furthermore, the elevated levels of SARS-CoV-2 IgG antibodies and the notable improvement in the clinical syndrome with oral corticosteroid treatment, along with the sustained remission, suggest a temporary immune dysregulation triggered by SARS-CoV-2.
In conclusion, we present a unique case that has not been previously reported, where a patient with a familial predisposition to autoimmune disorders exhibited FUO in conjunction with cluster headache. It highlights an area of central nervous system-immune system interaction which is poorly understood. Physicians should exercise vigilance when evaluating patients who present with headaches along with other central nervous system symptoms, especially in those with recent COVID-19 exposure or infection history to ensure timely initiation of appropriate treatment.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Dr Aravind Reghukumar, MD
Head of Department,
Department of Infectious Diseases,
Government medical college,
Thiruvananthapuram, Kerala, India
Email: draravind13@gmail.com