Vagus Nerve Schwannoma
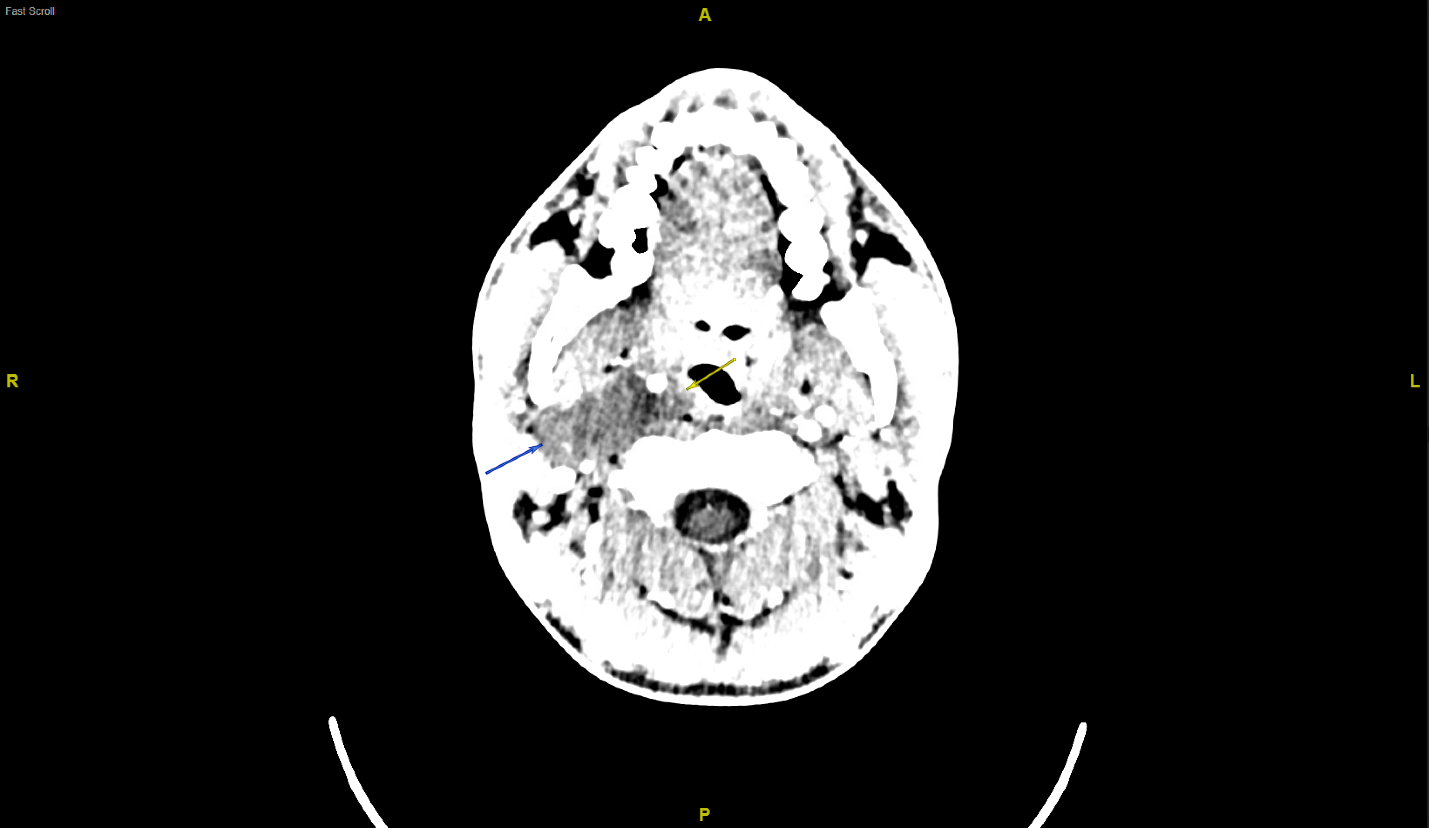
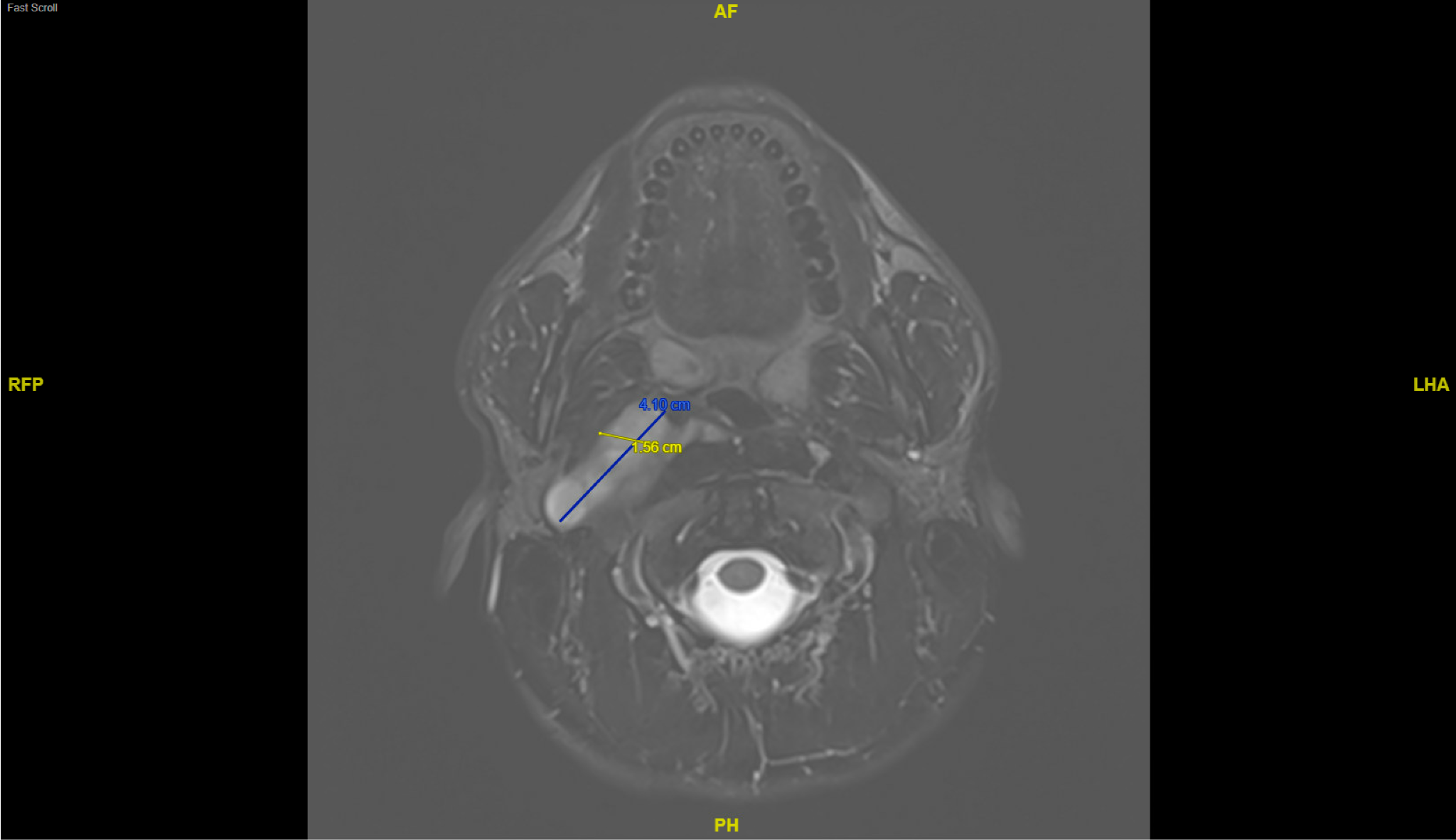
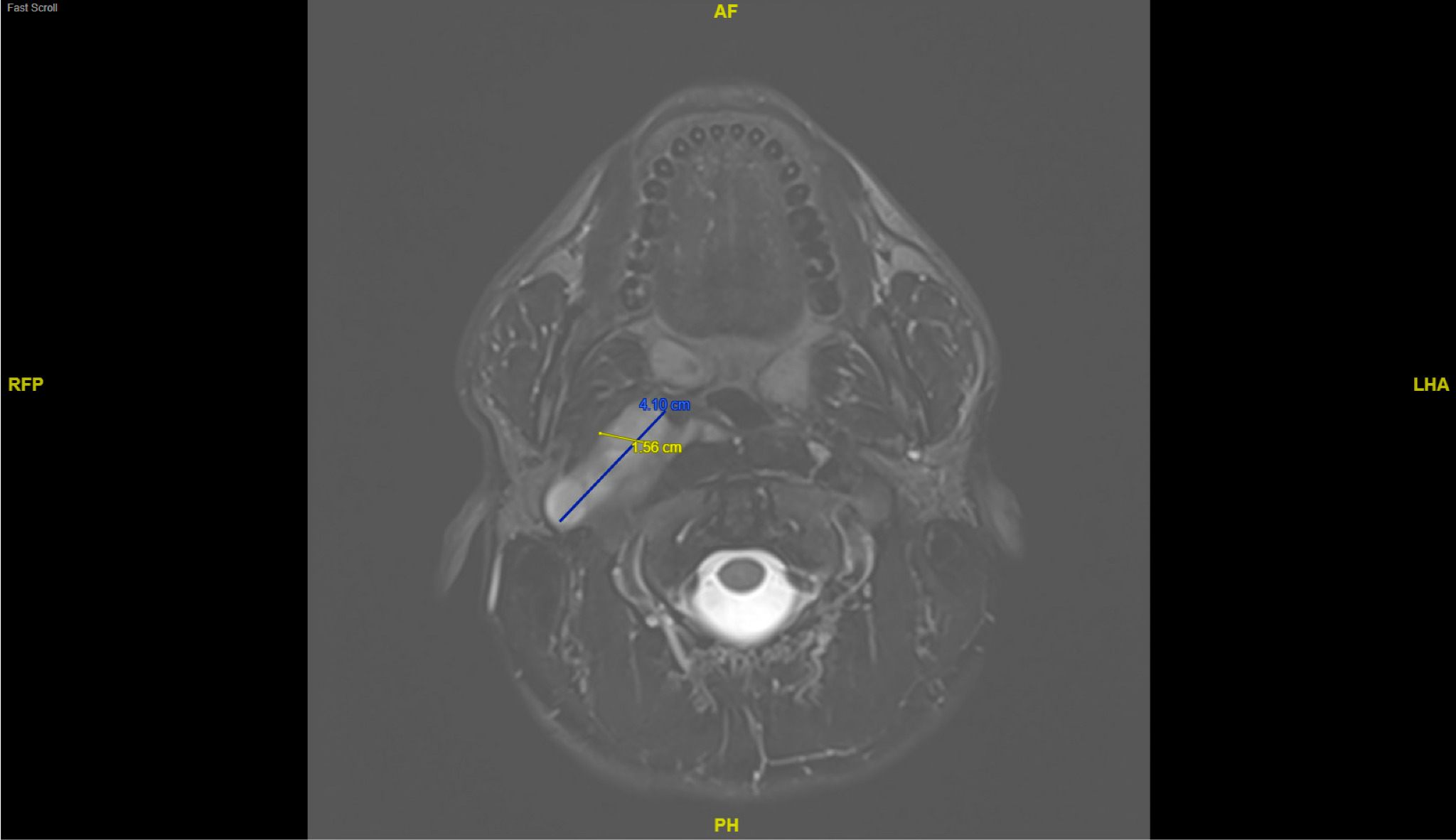
A 21-year-old previously healthy male presented with sudden-onset headache, photophobia, and neck pain accompanied by nausea and anxiety. Examination revealed right-sided neck tenderness to palpation and right-sided pain with active and passive movement. He had a normal cranial nerve and neurological exam without nuchal rigidity. Computerized tomography (CT) of the brain and neck showed a large cystic lesion in the carotid space (Figure 1). The lesion was further characterized with magnetic resonance imaging (MRI) that showed a 7.7 cm x 1.6 cm x 4.1 cm lobulated soft tissue mass involving the right carotid space with anterior displacement of the carotid artery. The lesion was isointense on T1-weighted imaging (T1WI), hyperintense on T2-weighted imaging (T2WI), and showed patchy internal enhancement concerning for a vagal nerve schwannoma (Figure 2).
Schwannomas are rare peripheral nerve tumors arising from the myelinating Schwann cells of the peripheral nervous system.1 Less frequently, they may impact cranial nerves. When affecting the vagus nerve, the patient may experience hoarseness or cough or may remain asymptomatic.2 Growth is usually limited to 2-3mm per year, and malignant transformation is possible but rare. Differential diagnosis of carotid space masses is broad but includes schwannoma of the vagus, glossopharyngeal, or spinal accessory nerves; congenital branchial cyst; paraganglioma; and infectious process.3,4 On MRI, paragangliomas usually show “salt and pepper” appearance due to flow voids, while branchial cleft cysts may show wall thickening, hypointensity on T1WI tending towards hyperintensity with infection or proteinaceous content, and variable intensity on T2WI.5,6 Schwannomas may appear cystic with isointensity on T1WI and hyperintensity on T2WI.1 Once schwannoma is suspected, the location of the internal carotid artery can provide diagnostic clues.7 Displacement of the internal carotid artery anteriorly away from the internal jugular vein is consistent with vagal nerve origin, and extension towards the jugular foramen of the skull further supports this diagnosis.2,7,8 Given encasement of upper cervical right internal carotid artery with anterior displacement, extension to the skull base, lack of internal flow voids disfavoring paraganglioma, and internal enhancement pattern disfavoring branchial cleft cyst, vagal nerve schwannoma was suspected and the patient was referred for surgical intervention.

Treatment is with surgical excision or debulking with nerve-sparing techniques when complete excision is not possible.2 Potential complications of excision include vocal cord palsy due to vagus nerve damage which may require subsequent nerve reconstruction.2 Progression may also lead to nerve deficit, pain, and compression of the carotid sheath structures. Prognosis is typically favorable with treatment.
Author contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Andrew Aultman
Warren Alpert Medical School at Brown University
Providence, RI, 02903
Email: Andrew_aultman@brown.edu