BACKGROUND
While the classic presentation of tuberculosis (TB) typically involves the pulmonary parenchyma, extrapulmonary tuberculosis (EPTB) remains an important manifestation of this disease and can involve almost any organ in the body. Despite its proximity to the lung, pleural manifestations of tuberculosis are classified as EPTB. After lymph nodes, the pleura is the second most common extrapulmonary site of involvement.1 Some classic risk factors for tuberculosis include immunocompromised state, diabetes mellitus, older age, occupational risk (stone workers), history of tobacco use, residing in areas where tuberculosis is endemic, and history incarceration.2 We discuss a case of a 65-year-old man without classic risk factors for tuberculosis who demonstrated several diagnostic challenges that emphasize the need for high clinical suspicion for EPTB in patients with recurrent pleural effusions.
CASE PRESENTATION
A 65-year-old male with a history of diabetes mellitus and atrial fibrillation presented to an outside hospital two months before presentation with decreased exercise tolerance and left-sided flank pain. At that time, he was found to have a left-sided exudative pleural effusion with a lymphocytic predominance and a spontaneous splenic hematoma thought to be due to anticoagulation with apixaban for atrial fibrillation. Initially, the effusion was suspected to be secondary to irritation of the diaphragm from the splenic hematoma given the timing of his symptoms. Despite embolization of the splenic artery by interventional radiology at the outside hospital the fluid continued to reaccumulate, and the patient required weekly therapeutic thoracentesis.
Because of the persistent pleural effusion, the patient underwent evaluation for active TB and was placed on airborne precautions. When the preliminary evaluation was negative with three acid-fast bacilli (AFB) smears and two Mycobacterium tuberculosis (MTB) PCRs, he underwent bronchoscopy with bronchoalveolar lavage (BAL). All diagnostic work up, including fungal and bacterial cultures, was negative. Given his extensive negative workup and clinical stability, he was discharged with follow up in general surgery clinic for possible splenectomy.
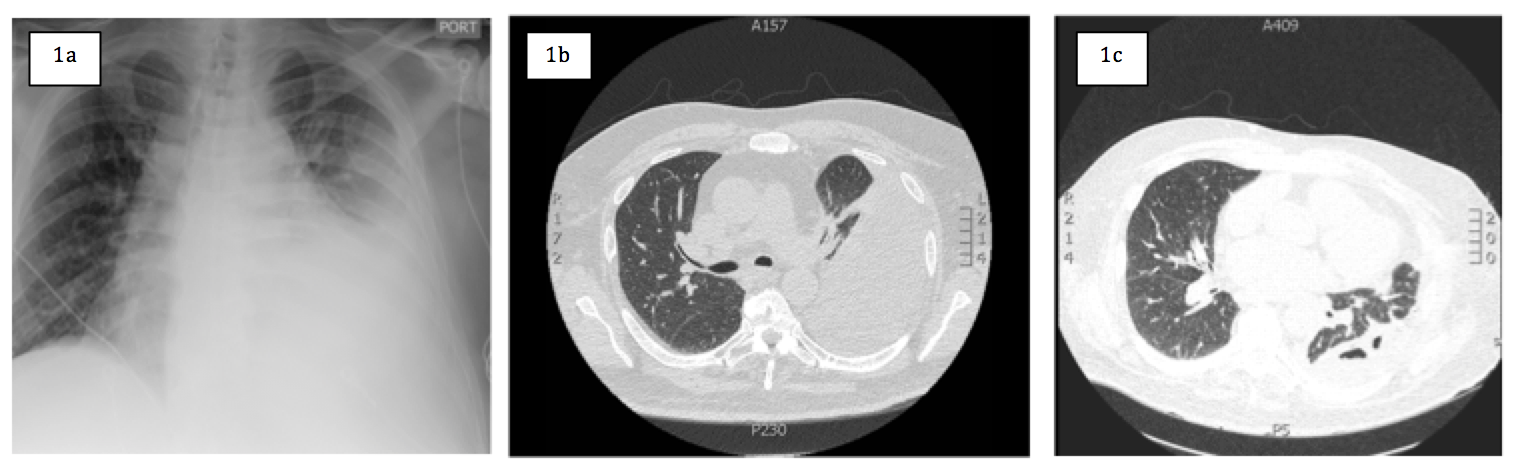
On arrival to the hospital, the patient presented with worsening dyspnea, fatigue, decreased appetite, and a progressively worsening dry cough. He endorsed a 25-pound weight loss since three months prior to admission, but denied any associated fevers, chills, or hemoptysis. He denied any His physical exam revealed decreased breath sounds in the left hemithorax, dullness to percussion at the left lung base, and mild tenderness to palpation in the left upper quadrant of the abdomen. A chest radiograph and computed tomography (CT) of the chest demonstrated a large left-sided pleural effusion (Figure 1a, 1b).
_chest_x-ray_at_presentation_to_our_institution_demonstrating_a_large_left-sided_pleural.png)
Given his history of lymphocytic-predominant exudative pleural effusions, the differential focused on possible infectious and malignant processes. The 4th generation HIV test obtained on admission was negative. A serum interferon γ-release assay (IGRA) was negative. A diagnostic thoracentesis was performed, and a left-sided chest tube was placed for symptomatic relief. Three liters of serosanguinous fluid was drained, and the patient reported immediate improvement in symptoms. Pleural fluid studies once again revealed an exudative effusion with a lymphocytic predominance. Gram stain and AFB smears were negative. Other studies were as follows: glucose 126 mg/dL, pH 8.2, adenosine deaminase 10 U/L, lactate dehydrogenase 66 U/L, protein 3.9 g/dL, and triglycerides 3.1 mg/dL. Pleural fluid bacterial cultures, fungal cultures, and AFB smears were negative. Coccidioides immunoglobulin G and immunoglobulin M enzyme immunoassay and histoplasma urinary antigen were negative.
After chest tube placement, a repeat CT chest demonstrated a partially loculated residual pleural effusion (Figure 1c). Because of high clinical suspicion for pleural TB or malignancy, the patient underwent diagnostic thoracoscopy and pleural biopsy by cardiothoracic surgery. Intraoperatively, one liter of purulent material was visualized and drained in the left hemithorax. After washout of the abscess cavity, a pleural biopsy was sent for evaluation, and samples were sent for bacterial, fungal, and AFB smear and culture. Gram stain of the purulent material obtained intraoperatively did not show any organisms, and post-operative chest tube output appropriately down-trended. The chest tube was removed on post-operative day five without issues, and the patient was discharged home with appropriate follow up. Cultures of the pleural abscess fluid continued to show no growth.
Further investigation of the pleural biopsy revealed small acid-fast bacilli with Ziehl-Neelsen (ZN) stain, no granulomas were seen, and the case was sent to an outside laboratory for expert consultation and final diagnosis. Immunohistochemistry (IHC) results of the pleural biopsy sample were positive for MTB. AFB cultures from the pleural biopsy were negative for MTB. It remained unclear whether the pathology represented active infection or previous infection with mycobacterium, but given the patient’s recurrent pleural effusions, he was started on rifampin, isoniazid, pyrazinamide, and ethambutol (RIPE). After clearance from the public health department, the patient was discharged home.
DISCUSSION
Pleural TB is challenging to diagnose due to nonspecific characteristics of the pleural fluid and a paucity of bacilli.3 The traditional diagnostic methods of tuberculin testing, ZN staining, and culture of pleural fluid samples for pulmonary TB have poor sensitivity in the evaluation of pleural TB.3,4
The gold standard for diagnosis of pleural TB is culture of the pleural biopsy specimen. However, additional diagnostic tools can potentially be used to narrow the differential diagnosis. Specifically, adenosine deaminase (ADA) and interferon-gamma (IFN- γ) levels within pleural fluid have consistently demonstrated high sensitivity and specificity for identification of EPTB cases.5,6 In a meta-analysis performed by Greco et al. involving 31 studies on ADA and 13 on IFN- γ, pooled sensitivity and specificity were 92% (range 56-100%) and 89% (range 55-100%) for ADA and 87% (range 57-100%) and 97% (range 90-100%) for IFN- γ, respectively. Though these tools are not considered gold standard for diagnosis, they provide a fast, non-invasive alternative that could be performed in most clinical laboratories.5 Non-specific markers of inflammation and immune response within pleural fluid, such as lysozyme and neopterin, have also demonstrated utility in differentiating malignant vs. tuberculous effusions, however their sensitivity and specificity have not been shown to be superior to ADA or IFN- γ.6
In order to facilitate the use of ADA levels in clinical practice, algorithms have been developed to guide its interpretation. Jeon et al. suggest using ADA as a screening tool, with levels >70 U/L being sufficient for treatment initiation and levels between 40 – 70 U/L requiring pleural biopsy. They suggest that values <40 U/L may preclude the need for continued investigation for TB altogether. However, our patient’s ADA level of 10 U/L demonstrates that pleural biopsy remains an important consideration when clinical suspicion for EPTB is high. In the future, combining ADA levels with other diagnostic tools may prove beneficial. For example, a study by Villegas et al. evaluated 42 cases of confirmed pleural TB and demonstrated that the combined use of ADA levels, polymerase chain reaction (PCR), and IFN- γ levels allow for a more sensitive and efficient diagnosis of pleural TB.3
IHC has shown increasing utility for quickly identifying MTB in tissue specimens with low bacillary load.7 In a study of 100 suspected cases of extrapulmonary EPTB, Kohli et al. demonstrated that IHC staining using polyclonal antibody to MTB identified 72% of cases compared to 23% identified by ZN staining.7 Given the increased sensitivity compared to ZN staining and relatively simplistic and cost-effective methodology compared to PCR, IHC may be particularly useful in low- and middle-income countries where cases of EPTB often go undiagnosed.8
Several proposed treatment regimens exist for pleural TB with an overarching goal to prevent the development of active pulmonary TB, reduce re-accumulation of pleural fluid, and prevent the development of long-term sequelae. In a study of 85 patients with pleural TB, Han et al. demonstrated that 49% of patients with significant pleural effusions at presentation had resolved by the end of 6 months of treatment.9 In addition, patients with residual disease continued to have improvement even after completion of six months of anti-TB medication.9 Loculation of pleural fluid on initial imaging predicted a higher risk of significant residual disease at two years follow up.9
Residual pleural thickening is a potential long-term sequela of pleural TB despite completion of treatment. In a study by Candela et al., 10% of patients with pleural TB who were correctly treated experienced mild to moderate restrictive pulmonary impairment.10 Investigation of the pleural fluid contents demonstrated that individuals who experienced restrictive functional sequelae had effusions with higher concentrations of cholesterol and triglycerides and a higher percentage of lymphocytes.10 These indicators of pleural inflammation may allow for the identification of individuals who are more likely to experience long-term pulmonary problems, but more research is needed to determine their clinical utility.
In patients such as ours with loculated effusions, several studies have examined the role of finbrinolytic agents to decrease residual thickening and improve long-term outcomes.11,12 Chung et al. compared loculated tuberculous pleural effusions irrigated with either saline or streptokinase over 3 consecutive days. After a year of follow up, the streptokinase group showed a significant improvement in forced vital capacity and lower occurrence of pleural thickening.11 Pending further research and investigation of long-term outcomes, the use of fibrinolytics may prove to be a safe and cost-effective option for management of loculated effusion in cases of pleural TB in the future.
In conclusion, this case highlights the diagnostic challenges specific to cases of EPTB. Most importantly, it demonstrates that in immunocompetent individuals without classic risk factors who present with an exudative, culture-negative effusion, the diagnosis of pleural TB must be considered. Even with a normal ADA in pleural fluid, physicians should consider alternative strategies for diagnosis including IHC, PCR, or novel biomarkers mentioned above. This case report highlights the need for deeper investigation with these tools to expedite diagnosis for these patients to decrease morbidity.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Corresponding Author
Satya Patel, MD, FACP
Assistant Clinical Professor, David Geffen School of Medicine at University of California, Los Angeles
Hospitalist, Greater Los Angeles Veterans Affairs Healthcare System
11301 Wilshire Blvd Bld 500 Mail Code 111 Los Angeles, CA 90073
Telephone: 310-478-3711 ext 44680
E-mail: satya.patel2@va.gov