
Background
Tracheal tumours are a rare entity, with an incidence of about 0.1 per 100,000 population. They can either arise from the trachea, known as primary tracheal tumours, or due to local invasion from nearby structures, such as the lung, larynx, esophagus, or thyroid gland. Malignant tracheal tumours are more common in adults, especially squamous cell carcinomas and adenoid cystic carcinomas, commonly identified as primary tracheal carcinoma.1 Primary tracheal adenoid cystic carcinoma (TACC) ranks as the second most prevalent tracheal malignant tumour, following squamous cell carcinoma, comprising roughly 10–20% of all tracheal malignancies. TACC originates from submucosal glands, demonstrating an indolent nature marked by slow growth and delayed distant metastasis.2 We present a case of a tracheal mass in a young woman who was misdiagnosed with asthma due to the indolent nature of the mass and delayed presentation.
Case Presentation
A 35-year-old woman with a previous history of exposure to biomass fuel (chullah/firewood) for around eight years came with a complaint of shortness of breath for 1.5 years and cough for eight months. There was no postural or diurnal variation of symptoms. She denied fever, weight loss, loss of appetite, or chest pain. The patient was previously diagnosed with asthma and was on multiple inhaler therapy (Formeterol/Budesonide/Tiotropium/add-on levo-salbutamol). Since there was no discernible improvement in her symptoms despite trying various inhalers, she was referred to our institution for a thorough evaluation and subsequent management.
On examination, her vital signs included oxygen saturation of 95% on room air, pulse of 100/min, and BP of 124/84mmHg. On examination, her breathing was labored; auscultation revealed a monophonic wheeze throughout the lung fields. Following a thorough history and clinical examination, the persistence of symptoms despite multiple inhalers and a monophonic wheeze led us to investigate alternative diagnoses. We considered the following differential diagnoses: extrinsic intrathoracic airway compression, tracheomalacia, bronchomalacia, tracheal/laryngeal stenosis, and luminal obstruction.
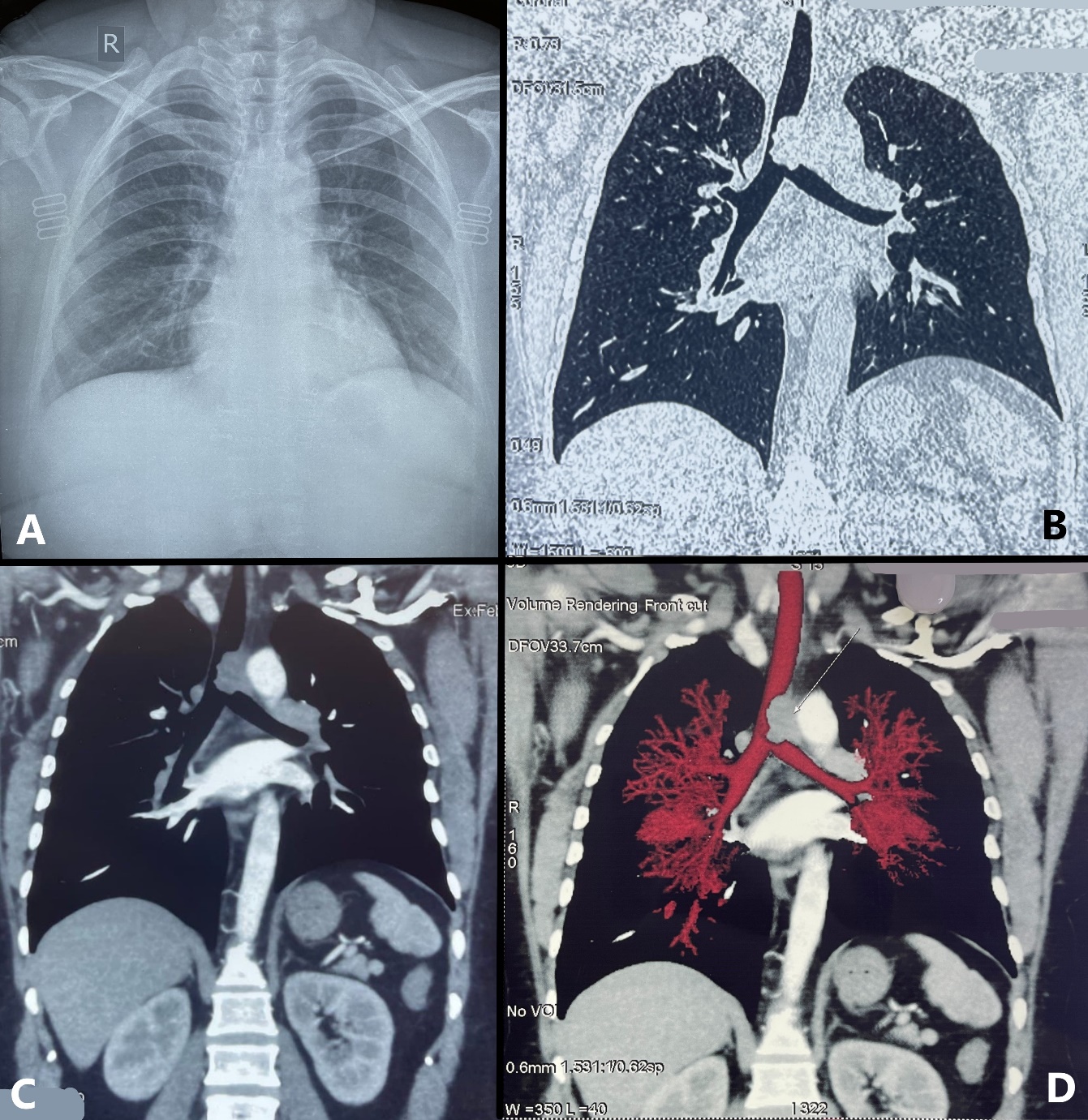
The chest radiograph showed a subtle haziness in the distal part of the trachea (Figure 1A). The routine investigations were within normal limits, including complete hemogram, liver function, and kidney function tests. Spirometry showed normal inspiratory limb with expiratory loop plateau suggestive of variable intrathoracic upper airway obstruction [FEV1 (L): 0.56, FVC (L): 1.94, FEV1/FVC: 28.9%, peak expiratory flow(L/S): 0.84]. Empey’s index [FEV1 (ml)/peak expiratory flow rate(l/m)] was found to be 11.11 (>8), which is again suggestive of upper airway obstruction. Computerized tomography (CT) of the thorax revealed a well-defined polypoidal soft tissue mass (2.6x2.0x1.8cm) arising from the left lateral wall of the distal trachea just above the carina, causing marked narrowing of the distal trachea and the left main stem bronchus (Figure 1B-D). PET-CT also revealed the same findings with a standardized uptake value (SUV) max of 5.5 and no metastasis.
_showing_subtle_opacity_in_distal_trachea__cect_thorax___b-_lung_w.jpeg)
On bronchoscopy, a polypoidal growth was seen in the distal trachea originating from the left lateral tracheal wall, almost obliterating 70% of the lumen (Figure 2A&2B), and the vascularity was assessed using narrow band imaging (Figure 2C). Histopathological examination of the cryobiopsy specimen (Figure 2D) revealed a subendothelial tumor characterized by cribriform glands lined with round to oval-shaped cells containing luminal mucin, confirming the diagnosis of adenoid cystic carcinoma. Due to the extension of the mass into the left main bronchus and the non-feasibility of surgery, the patient was referred for combined chemoradiotherapy.

Discussion
Primary tracheal carcinomas are rare tumours with an incidence of 0.1 to 0.26 per 100,000 people, accounting for 0.1-0.4% of all malignant diseases.2 The most prevalent histology among them is squamous cell carcinoma, followed by adenoid cystic carcinoma (ACC), undifferentiated carcinoma, small cell carcinoma, adenocarcinoma, large cell carcinoma, and sarcoma.3 According to the epidemiologic studies, ACC is the second-most common primary malignant tracheal tumour, occurring in 10–15% of cases.1 They resemble salivary gland tumours, which are well differentiated and slow-growing; they may infiltrate submucosal planes circumferentially and longitudinally along the airway axis far beyond the gross lesion because of their lack of capsule.4 Both sexes are affected equally in the fourth to fifth decade of life. While smoking is an identified risk factor for squamous cell carcinomas, ACC does not appear to have a relation with smoking status.1 ACC usually presents with symptoms of mass effect that include cough, wheezing, and dyspnoea, which are commonly misdiagnosed as asthma or chronic obstructive pulmonary disease and often would have received treatment for the same.5 It is, therefore, common for these diseases to be diagnosed late, after one year of symptom onset. They have an indolent course but recur in the later stages.1
Tracheal neoplasms are notoriously difficult to visualize on routine radiography. Characteristic CT findings consist of a polypoid or sessile, intraluminal mass of soft tissue density. Malignant and benign tumours may be differentiated if the former shows local invasion into surrounding structures. Newer techniques in bronchoscopy, like narrow-band imaging (NBI), are available in diagnosing lung cancers. NBI employs a specialized filter to eliminate broadband light across the RGB (red-green-blue) spectrum, isolating the narrow band spectrum (blue and green). Subsequently, the retained narrow-band is utilized: the blue narrow-band light illuminates the capillaries of the surface mucosal layer. In contrast, the green narrow-band light enables visualization of the thick blood vessels within the mucous membranes. The merits of NBI in lung cancer diagnoses lie in its ability to concurrently capture the morphology of bronchial mucosa and the epithelial vascular network. The synergy of these two bands generates exceptional contrast on the mucosal surface, streamlines examination processes, and reduces the need for non-productive biopsies.6 Nevertheless, its application in central airway tumours is limited, even though it can offer insights into the vascularity of the tumour.
Surgery is the mainstay of management. It should be avoided in cases where there is a regional invasion of neighbouring organs or major blood vessels, extensive mediastinal lymph node involvement, presence of distant metastases, or a history of high-dose (>50 Gy) irradiation to the trachea.1 Prognosis of ACC of the trachea is generally good. The rates of successful complete resection range from 42% to 57%. For cases with advanced tumour stage (T4), incomplete surgical resection (R1 and R2), or perineural invasion (Pn1), a multimodal treatment approach is recommended. Adjuvant radiotherapy after surgery is the preferred strategy in such cases.7 Patients who are ineligible for surgery or radiotherapy can explore alternative treatments like bronchoscopy ablation and stent placement. Bronchoscopic interventional techniques, including transbronchial cryotherapy, high-frequency electrocautery, laser, and argon plasma coagulation, can rapidly alleviate clinical symptoms and prolong survival. However, their extended treatment duration and potential complications may contribute to recurrence.8 Airway margins, radial resection, and lymph node metastases are important prognostic factors for survival.4 The 5-year prognosis is better in patients with intraluminal involvement (50%) compared to extraluminal spread (18%).9 In our case, an extension of the mass into the left main bronchus rendered the patient non-feasible for surgery and hence referred for combined chemoradiotherapy.
In summary, wheezing often presents as the predominant symptom of ACC, closely resembling asthma and potentially leading to significant delays in diagnosis, typically averaging about 12 months. It is crucial for physicians to recognize that if interventions aimed at presumed asthma yield no improvement, additional exploration, such as imaging or consultation with pulmonology specialists, may be necessary.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Corresponding Author
Vinay V
DM Fellow
Department of Pulmonary, critical care and sleep medicine
All India Institute of Medical Sciences, Patna, INDIA
Email: docvinayv@gmail.com