

BACKGROUND
During embryonic development, the thyroid gland descends along the thyroglossal duct from the blind foramen to its anatomical position in the anterior portion of the trachea.1 Occasionally, errors occur during gland migration, resulting in what is known as ectopic thyroid tissue.2 A disruption at the beginning of migration results in thyroid tissue at the base of the tongue, the most common location (90%).1,3 Similarly, incomplete migration results in high cervical thyroid tissue, while excessive migration may result in mediastinal (<1%)4 or pericardiac1 thyroid tissue. Other locations include the palatine tonsils, axilla, descending aorta, gastrointestinal system, adrenal gland, and reproductive system.2 We present a woman in the Dominican Republic with dual ectopic thyroid that was incidentally discovered.
CASE PRESENTATION
A 69-year-old woman with a known history of hypertension, type 2 diabetes, and untreated thyroid goiter diagnosed seven years ago was evaluated by the gastroenterology department due to a history of dyspeptic symptoms, asthenia, aphonia, and chronic fatigue. The patient was referred to the internal medicine department for pre-anesthesia evaluation before undergoing an upper gastrointestinal endoscopy. Physical examination showed a symmetrical, cylindrical neck with a mass with irregular borders in the anterior region. Routine laboratory tests and chest radiographs were indicated for pre-procedural evaluation. The chest radiograph showed tracheal deviation to the right. Therefore, other imaging studies were conducted. Ultrasonography findings revealed a multinodular thyroid goiter with cystic degenerations inside. The right lobe was 1.7 cm x 1.2 cm x 1.0 cm with a volume of 1.14 mL and a left lobe of 3.6 cm x 3.5 cm x 2.7 cm with a volume of 18.8 mL. Computed tomography (CT) scan of the neck and chest showed an intrathoracic thyroid goiter with associated calcifications, which caused the trachea and esophagus to be displaced to the right.
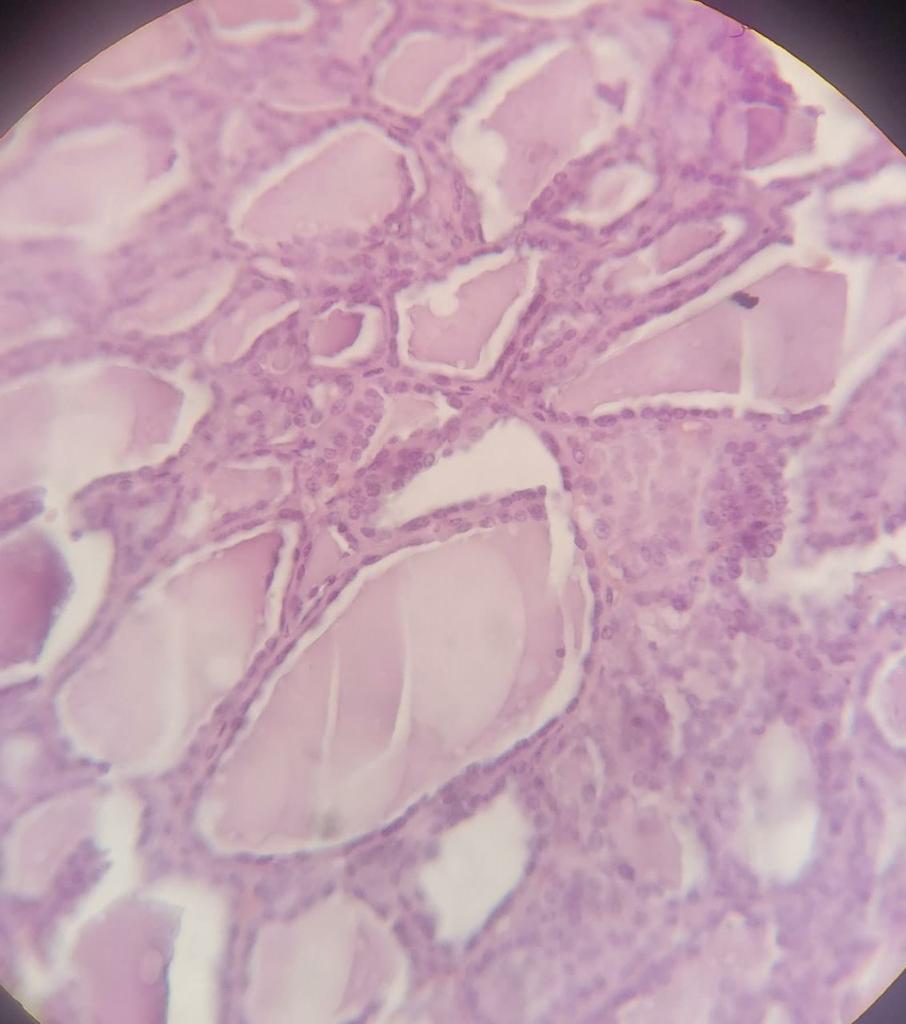
Laboratory work revealed a TSH level of 0.350 mlU/L (range: 0.3-4.2 mlU/L) and free T4 of 20.47 pmol/L (range: 12-22 pmol/L). Endocrinology referral for a biopsy of the mass was initially considered. However, due to the intrathoracic location of the mass and the presenting complaints, referral to the surgery department was prioritized. The patient underwent radical thyroidectomy and dissection (Figure 1) with subsequent biopsy of the mass, which yielded the following diagnoses: 1) benign follicular hyperplasia (multinodular goiter), 2) ectopic thyroid tissue with associated benign follicular hyperplasia (cervical goiter) (Figure 2A), 3) ectopic thyroid tissue with focal adenomatous changes within a context of benign follicular hyperplasia (mediastinal goiter) (Figure 2B). During follow-up, the patient’s dyspeptic symptoms had resolved, and the thyroid profile showed a TSH level of 6.90 mlU/L (range: 0.3-4.2 mlU/L). The patient was started on levothyroxine.
_product_of_total_thyroidectomy._the_right_lobe_measured_4.5_cm_x_3_cm_x_2_cm__the_i.jpeg)
_histology.jpeg)

DISCUSSION
Thyroid ectopia cases occur in 1 per 100,000 to 300,000 persons in the general population, with a female-to-male ratio of 3-4:13. Likewise, the prevalence within the population with thyroid disease is 1 per 4,000 to 8,000 persons.3 Although in most cases (47%) it is asymptomatic, it can present with dysphagia, dysphonia, hypernasality, cough, foreign body sensation, hemoptysis, and stridor, among others.2,5 Treatment is dependent on the patient’s presentation. Asymptomatic euthyroid patients do not usually require treatment and are kept under observation. For hypothyroid patients, treatment is with thyroid hormone replacement.3 Surgical removal of the gland is the preferred approach in cases of hemorrhage, ulceration, obstructive symptoms, uncontrolled hyperthyroidism, and malignant neoplasia.2 In most cases, the diagnosis of malignancy is reached after excision and biopsy of the mass. While rarely documented, there exists a less than 1% estimated risk of malignant transformation from ectopic thyroid tissue, with papillary carcinoma being the most prevalent subtype.2,5 Other complications associated with thyroid ectopia include benign neoplasia, thyroiditis, and hypothyroidism.2
Based on a literature review of 25 cases,6–31 31 patients were identified to have ectopic thyroid tissue. Of the 31 patients, 22 (70.97%) were female, and 21 (67.76%) were 18 years or younger, with a median age of 14, ranging from 4 to 75 years. While most cases are typically identified through neonatal screening, it is noteworthy that in the Dominican Republic, thyroid studies are not routinely done as part of neonatal screening protocols due to their unavailability unless specifically requested by parents, particularly in private healthcare settings. It is essential to consider that ectopic thyroid tissue may undergo enlargement during periods of stress, potentially leading to symptomatic presentations later in life, as observed in this case.2
Regarding the location of the ectopic tissue, 26 (83.87%) of the patients had ectopia at the base of the tongue/lingual area. Other common locations included the sub-hyoid area (n=15, 48.39%), supra-hyoid (n=6, 19.35%), and the area anterior to the thyroid notch, submental region, and pre-hyoid with 9.68% each. The least frequent locations were the liver, the pre-tracheal area, the submandibular area, and the right paramedian line, as well as more unspecific locations, such as the floor of the mouth and neck, present in one patient each. During thyroid examination, the most common finding was swelling of the anterior line of the neck (n=23, 74.19%), followed by absent thyroid tissue in its usual location on palpation (n=4, 12.9%), lateral neck mass (n=1, 3.23%), whereas three (9.68%) of patients had a regular thyroid exam. Among the associated symptoms, five (16.13%) patients reported dysphagia, three (9.68%) odynophagia, and two (3.23%) reported hoarseness, cough, and dysphonia. Other symptoms listed included foreign body sensation, pain, and unspecific symptoms of hypo/hyperthyroidism. Regarding the chemical evaluation of thyroid function, TSH was normal in eight (25.81%) and elevated in twenty-one (67.74%) patients. Among the cases that reported fine needle aspiration (n=12, 38.71%), the findings included follicular cells (n=7, 58.33%) and colloid (n=3, 25%).
In conclusion, the presented case of dual ectopic thyroid tissue showcases this anomaly’s remarkable rarity and diagnostic challenges. Recognizing the multifaceted nature of ectopic thyroid presentations is crucial for accurate diagnosis and appropriate management, especially in countries with limited or unavailable newborn screening. In such settings, heightened awareness, and expertise in recognizing the different presentations become imperative for healthcare practitioners to navigate the challenges posed by limited screening resources, ultimately contributing to enhanced healthcare delivery, and improved overall public health. This case adds to the limited literature, emphasizing the need for thorough investigation in complex clinical presentations.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors authorship criteria.
-
Substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures
The authors have no conflicts of interest to disclose.
Corresponding Author
Noemí Acevedo
510 W 45th, Manhattan, NY, 10036
Phone: +1 (829) 876 – 8197
Email: n.acevedo@ce.pucmm.edu.do