



Background
Renal papillary necrosis is thought to be due to ischemic damage to the medullary region of the kidney.1 This can lead to papillary tissue damage and subsequent sloughing of the dead tissue into the urine, obstructing the collecting system (pelvicalyceal system) and resulting in hydroureteronephrosis. The sloughed-off renal papilla is passed as large flaky tissue in urine. Papillary necrosis has been described in analgesic nephropathy, urinary tract infection, sickle cell disease, uncontrolled diabetes mellitus, calyceal arteritis, and necrotizing angiitis.2 Candida-associated renal papillary necrosis is very rarely reported in the literature. Growth of Candida in urine culture in a patient with diabetes mellitus is often neglected as it is thought to reflect contamination. We describe two patients who presented with hydroureteronephrosis and were diagnosed with candida associated renal papillary necrosis following severe COVID-19 infection (Figure 1).

Case 1
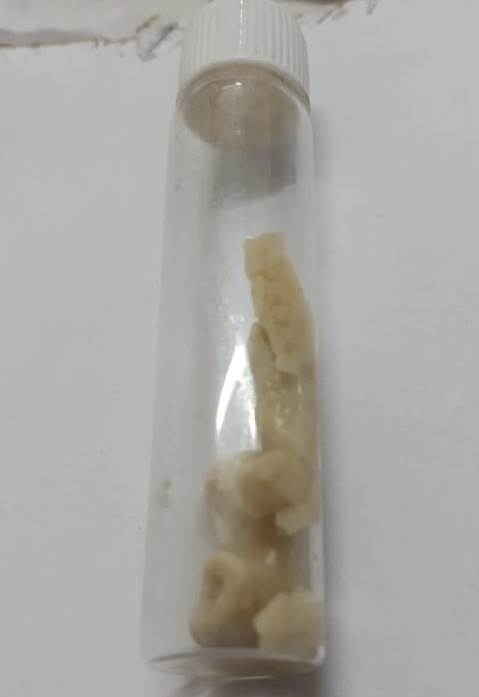
A 50-year-old man with a history of long-standing diabetes mellitus presented to the hospital with abdominal pain and dyspnea. Eight months prior to his current admission, he had been treated for severe COVID-19 pneumonia and pulmonary embolism with corticosteroids, tocilizumab, and systemic anticoagulants. The cumulative doses used during the treatment of COVID-19 were 400 mg of methylprednisolone and 400 mg of tocilizumab. Serum creatinine level was noted to be 1.4mg/dl (normal range 0.5-1.4 mg/dl) two months prior to admission. Before the diagnosis of SARS-CoV-2 infection, there was no history of renal dysfunction, nephrolithiasis, or urinary tract infection. At admission, serum creatinine was 4.4mg/dl, and sonography of the abdomen and pelvis showed right hydroureteronephrosis with no evidence of nephrolithiasis. The patient passed milky urine with large amounts of flaky tissue (Figure 2), which was confirmed to be necrotic renal papilla by histopathology (Figure 3). Potassium hydroxide (KOH) stain showed the presence of fungal elements in the necrotic renal papillary tissue, and culture grew Candida tropicalis. Previous urine cultures had grown multiple organisms, including E. coli and Klebsiella, at various times during the previous eight months. The patient underwent DJ ureteral stenting and was treated with fluconazole according to susceptibility testing. His renal function improved, and papillary tissue stopped appearing in the urine. Subsequently, urine culture also grew Mycobacterium tuberculosis. At present, the patient is on anti-tuberculous therapy (ATT) and fluconazole with a serum creatinine of 1.8mg/dl. Urine culture showed persistence of fluconazole-susceptible Candida tropicalis for eight months, and fluconazole 400mg daily was continued for eight months, after which creatinine stabilized and urine culture became sterile.


Case 2
A 55-year-old-man with diabetic kidney disease, chronic kidney disease (CKD stage 4), retinopathy, and coronary artery disease with a baseline serum creatinine level of 4.4 mg/dl, estimated glomerular filtration rate (GFR) 16ml/min, was admitted with severe COVID-19 pneumonia. He had hypoxia, for which he was administered intravenous (IV) methylprednisolone 40mg twice daily. As the serum creatinine increased to 8 mg/dl with oliguria, he was initiated on hemodialysis. He improved clinically, and immunomodulators were reduced. After seven days, IV steroids were converted to oral deflazacort 6mg thrice a day, tapered every five days. Ten days later, he started passing fleshy tissue in urine and developed acute urinary retention requiring Foley catheter insertion. Tissue passed in urine showed papillary necrosis with Candida on histopathological examination. Urine culture grew Candida parapsilosis (Figures 4, 5). He was started on intravenous followed by oral fluconazole based on antimicrobial susceptibilities. Serum creatinine levels improved from 6.7mg/dl to 5.4mg/dl. Ultrasonography did not show calyceal obstruction at the time. The patient was given two weeks of fluconazole, after which he did not have a recurrence of the symptoms, and further urine cultures remained sterile. One month later, he developed multidrug-resistant (MDR) Klebsiella infection and septic shock with acute kidney injury. He recovered and was continued on maintenance hemodialysis.


Discussion
With the coming of COVID -19 pandemic, invasive fungal infections (IFI) have become more common than in the past.3 Invasive candidiasis, comprised of candidemia and deep-seated tissue candidiasis, is the most common fungal illness among hospitalized patients in the developed world.4 Candiduria, by itself, is widespread in hospitalized patients, especially those with predisposing factors, including diabetes mellitus, indwelling urinary catheters, and exposure to antimicrobials.5 Most patients with candiduria may be asymptomatic and likely reflect colonization rather than infection. Such patients may benefit from removing the predisposing factors like catheters or correcting an underlying immunosuppressed state. Renal involvement from candida can be either secondary to ascending infection from the lower urinary tract or seeding due to candidemia. Asymptomatic candiduria does not warrant treatment except in the presence of severe neutropenia or in case a urological manipulation is being planned. Symptomatic candiduria should be treated.6 Development of fungal balls may require surgical removal.
Renal papillary necrosis is characterized by coagulative necrosis of the renal papilla and the background medullary pyramids.2 It was first described by Friedrich in 1877, although the autopsy in 1827 of the Austrian composer Ludwig Van Beethoven contained a similar pathological description that has been attributed to long-term analgesic use.7,8 The necrotic foci may get infected and can be expelled as sloughed papillla in urine. Necrotic papilla can cause tubular obstruction, which, when bilateral, can lead to renal failure. Infected papillary necrosis may be fatal.2 Candida-associated renal papillary necrosis was first described in 1981.9 The primary reported association was immunosuppression due to drugs or extreme prematurity in infants. These cases were from autopsy findings, with no case being diagnosed antemortem, probably because imaging at that time was not as developed and freely available as it is today. There are only a few described cases of candidal papillary necrosis.10 In an isolated case reported in 2003, a patient was described with bilateral ureteral obstruction due to candidal fungal balls and improved with prolonged treatment with fluconazole and ureteroscopic removal of the necrotic tissue.11 The risk factors for fungal infection were diabetes mellitus and neurogenic bladder. Candidal papillary necrosis has also been reported in renal allograft.12
COVID-19 infection causes immune dysregulation, possibly due to interference with proinflammatory markers, interferon, cytokine levels, and altered function of cells of innate immunity.13 The presence of COVID-19 infection itself may lead to an immunocompromised state. Treatment of severe COVID-19 infection and the associated cytokine storm involves the use of immunosuppressants such as corticosteroids, Interleukin-6 receptor inhibitor tocilizumab, and Janus kinase inhibitors such as tofacitinib and baricitinib, as per current guidelines. SARS-CoV-2 infection, as well as the use of corticosteroids, can also worsen the glycemic status of those with diabetes mellitus. An increase in COVID-19-associated invasive fungal infections has been observed, of which the most common infections are invasive candidiasis, COVID-19-associated pulmonary aspergillosis (CAPA), and COVID-19-associated mucormycosis (CAM).14 Among Candida infections, it has also been noted that the incidence of Candida auris, which is fluconazole-resistant, has increased.
In conclusion, the incidence of invasive fungal infections is increasing in the COVID-19 era. Fungal urinary tract infections, if recognized early, are a treatable and reversible cause of acute kidney injury. Clinicians should be aware of fungal urinary tract infection complications in patients with underlying immunocompromised states, mainly when bacterial urine culture is sterile or shows multiple organisms. Passage of a fleshy mass in urine may indicate renal papillary necrosis. History of SARS-CoV-2 infection and use of immunomodulators like corticosteroids, tocilizumab, and JAK inhibitors should prompt clinicians to consider Candida-related renal papillary necrosis.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of interest
The Authors declare no conflict of interest
Corresponding Author
Dr. Aravind Reghukumar
Head of department, Dept of Infectious Diseases
Government Medical College Hospital
Thiruvananthapuram
Email: draravind13@gmail.com